Download
1 / 31
310 likes | 473 Vues
PREGNANCY-RELATED MORTALITY ASSOCIATED WITH OBESITY IN FLORIDA 1999 THROUGH 2002. Daniel Thompson, M.P.H. Carol Graham, Ph.D. Florida Department of Health, Division of Family Health Services Bureau of Family and Community Health. In 1996 Florida initiated the

E N D
PREGNANCY-RELATED MORTALITY ASSOCIATED WITH OBESITY INFLORIDA 1999 THROUGH 2002 Daniel Thompson, M.P.H. Carol Graham, Ph.D. Florida Department of Health, Division of Family Health ServicesBureau of Family and Community Health
In 1996 Florida initiated the Pregnancy-Associated Review (PAMR) process to improve surveillance and analysis of pregnancy-related mortality.
The Florida Department of Health’s decision to develop a systematic approach to examining maternal deaths was prompted by: 1) CDC publications confirming the underreporting of maternal deaths; 2) Questions about the relationship of maternal deaths to changes that were occurring in healthcare delivery systems; and, 3) A cluster of maternal deaths observed in a Florida county.
The CDC and ACOG’s expanded definition of maternal mortality was adopted and includes, “death of a woman, from any cause, while she is pregnant or within one year of termination of pregnancy, regardless of duration and site of the pregnancy.”
In PAMR, pregnancy-associated deaths are reviewed by the PAMR review team. The review team is a multidisciplinary committee of 31 professionals: (physicians, nurses, nurse midwives, social workers, and researchers)
The review team meets quarterly to discuss abstracted records. They examine trends, common elements, and formulate potential strategies to address these factors. Team members volunteer their time and provide their own travel costs.
Each case is reviewed for issues relating to maternal mortality. Issues identified include: 1) Documented history of medical problems 2) Medical problems during pregnancy 3) Medical problems associated with labor and delivery 4) Medical problems during the postpartum period 5) Nutrition issues 6) Access to prenatal care 7) Substance use (continued on next slide)
8) Absence of prenatal risk assessment 9) Lack of social support 10) Problems with housing 11) Mental health problems 12) Family violence or neglect 13) Social issues 14) Access to transportation 15) Problems with provision or design of services 16) Environmental or occupational hazards 17) Concerns about family planning access or contraceptive method
After review, the team gives a final classification to each case as: • pregnancy-related, • possibly pregnancy-related, or • not pregnancy-related.
Case Identification The Division of Family Health Services, in collaboration with the Office of Planning, Evaluation, and Data Analysis, implemented selection criteria to maximize the identification of pregnancy-associated deaths. Women are included on the surveillance list of pregnancy-associated deaths by any of the following four ways:
Case Identification 1) The response on the death certificate is “yes” to the question, “If female, was there a pregnancy in the past 3 months?” 2) The ICD-10 code indicates a death classified as being due to, “Pregnancy, Childbirth, and the puerperium.”
Case Identification 3) There is a matching birth or fetal death record within 365 days prior to the woman’s death. 4) There is a matching Healthy Start Prenatal Screen (Florida’s universal prenatal screening tool used to assess risk and identify women most at risk for adverse health outcomes).
Case Abstraction Process The PAMR abstraction process is modeled after the NFIMR (National Fetal and Infant Mortality Review) process. Abstraction forms capture information from the medical and social history, prenatal, labor and delivery, postpartum, social service, care coordination, and terminal events records. FIMR abstractors are hired to review selected PAMR records in their areas.
143 deaths were classified by the PAMR review as pregnancy-related in Florida in the four year period 1999 through 2002. Anecdotal evidence reviewed in the PAMR process suggested that obesity might be associated with increased risk of pregnancy-related mortality. The purpose of this analysis is to quantify the relationship between obesity and risk of pregnancy-related mortality in Florida.
Matched Case – Control Analysis In case-control analyses: Cases are persons with the attribute of interest. Controls are persons that do not have the attribute of interest. Inferences are made by comparing cases to controls.
Matched Case – Control Analysis In this analysis, cases are pregnancy-related deaths and controls are women screened with the Healthy Start Prenatal risk screening. Cases and controls were pregnant and therefore, at risk for pregnancy-related death.
Matched Case – Control Analysis For each case, 4 matched controls were randomly selected from prenatal screening records for 1999 – 2002. The controls were matched to the cases based on education, age, marital status, and race. Matching is a method used to control for the confounding influence of these variables.
Matched Case – Control Analysis There were 143 PAMR deaths in Florida occurring in the years 1999 through 2002. For this analysis, 28 (20%) of these deaths were excluded due to missing data for height, weight, age, race, marital status, or education. This left 115 for analysis.
Matched Case – Control Analysis Pre-pregnancy height and weight data are on the PAMR record for cases and on the prenatal screening record for controls. These are used to calculate the body mass index (BMI) for cases and controls. The formula is: weight divided by the square of the height, where weight is in kilograms and height is in meters.
Matched Case – Control Analysis Cases tend to have higher percentages in the higher BMI categories, compared to the controls. Also, 25.2% of the cases are in the normal BMI category and 47.2% of the controls are in the normal BMI category.
Matched Case – Control Analysis Conditional Logistic Regression was used to calculate adjusted odds ratios, confidence intervals and p values. This method is used for matched, case-control data.
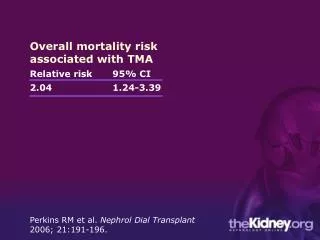
Matched Case – Control Analysis This table shows the adjusted odds ratios for pregnancy- related death associated with the BMI categories, using the “Normal Weight” category as the reference. All of the BMI categories are associated with increased risk of pregnancy-related death. (The Under weight category is borderline statistically significant) Additionally, the pattern follows a dose response trend with higher adjusted odds ratios associated with the higher BMI categories.
Limitations Missing values resulted in the exclusion of 20% of the cases. If the excluded cases were substantially different from the cases in the analysis, the results could be biased. Also, the BMI is based on self reported pre-pregnancy height and weight and there could be reporting bias since it is likely that people tend to under-estimate their weight.
Limitations However, if the reporting bias affects both cases and controls equally, the odds ratios will tend to not be affected since the biases cancel in the calculations.
Conclusions The adjusted odds ratios indicate that high BMI is associated with greatly increased risk of pregnancy related death. Since the cases and controls were matched, these odds ratios are not influenced by differences in race, age, education, or marital status between the cases and the controls.