HSV Encephalitis
HSV Encephalitis. Jack Kuritzky, PGY-2 UNC Internal Medicine August 31, 2009. HSV Encephalitis: General. Encephalitis: 20,000 cases/year HSV accounts for 10-20% HSV-1 causes encephalitis in adults HSV-1 or HSV-2 in neonates HSV-1 and 2 associated w/Mollaret’s meningitis

HSV Encephalitis
E N D
Presentation Transcript
HSV Encephalitis Jack Kuritzky, PGY-2 UNC Internal Medicine August 31, 2009
HSV Encephalitis: General • Encephalitis: 20,000 cases/year • HSV accounts for 10-20% • HSV-1 causes encephalitis in adults • HSV-1 or HSV-2 in neonates • HSV-1 and 2 associated w/Mollaret’s meningitis • Benign recurrent lymphocytic meningitis • Preferentially affects temporal lobe • Can rarely cause recurrent brainstem encephalitis • HSV-2 tends to cause global encephalitis • 1/3 cases <20yrs and 1/2 cases >50 yrs
HSV Encephalitis: Pathogenesis • Infiltrates CNS via 3 routes • 1. Trigeminal nerve or olfactory tract • Typically after primary infection • <18yrs old • 2. CNS invasion after recurrent infection • Viral reactivation w/subsequent spread • 3. CNS infection w/o primary or recurrent HSV-1 • Latent HSV in situ within CNS • Invades and replicates in neurons and glia • Causes necrotizing encephalitis • Widespread hemorrhagic necrosis throughout parenchyma
HSV Encephalitis: Pathogenesis • Necrosis of temporal lobe
HSV Encephalitis: Pathogenesis • Necrosis of temporal lobe • Immune mediated • Not more common in immunosuppressed • Small studies suggest HSV viral load does not correlate with degree of temporal lobe damage
HSV Encephalitis: Presentation • Fever • Altered mental status • Altered level of consciousness • Focal cranial nerve deficits • Hemiparesis • Dysphasia/aphasia • Ataxia • Focal seizures
HSV Encephalitis: Presentation • Fever • Altered mental status • Altered level of consciousness • Focal cranial nerve deficits • Hemiparesis • Dysphasia/aphasia • Ataxia • Focal seizures
HSV Encephalitis: Presentation • More on AMS – consequences of temporal lobe damage • Hypomania - elevated mood, excessive animation, decreased need for sleep, inflated self-esteem, and hypersexuality • Kluver-Bucy syndrome (KBS) • Initially seen in Rhesus monkeys • Loss of normal anger and fear responses • Increased sexual activity • Amnesia
HSV Encephalitis: Diagnosis • CSF • Lymphocytic pleocytosis • Erythrocytosis (84% of patients) • Elevated protein • Low glucose uncommon • CSF PCR now diagnostic test of choice • Quickest, sensitive, and specific • HSV culture out of favor • Brain biopsies previously performed
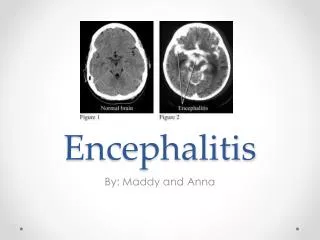
HSV Encephalitis: Diagnosis • Imaging • Temporal lobe injury
HSV Encephalitis: Diagnosis • Imaging – Temporal lobe injury • Usually unilateral • May have mass effect • MRI much more sensitive/specific • EEG – focal findings in >80% cases • High amplitude slow waves (delta and theta slowing) • Continuous periodic lateralized epileptiform discharges in the affected region
HSV Encephalitis: Treatment • EARLY TREATMENT IMPERATIVE! • Before loss of consciousness • Within 24 hours of the onset of symptoms • Glasgow Coma Scale score of 9 to 15 • Acyclovir 10 mg/kg IV Q 8h (infuse slowly to prevent crystalluria/renal failure) • Mortality 19-28% vs. 50-58% w/vidarabine • 6 month functional status significantly better w/acyclovir • Treat 14-21 days • Future treatment steroids? (non-randomized, retrospective study)
HSV Encephalitis: Prognosis • Untreated, mortality 70% • Survivors with severe neurologic damage • With treatment—mortality ~20%! • Severe disability in 20% • Simplified Acute Physiology Score II >/=27 • Delay >2 days b/w admission and acyclovir • GCS <6 • Age>30 • 62% of survivors have neurologic sequelae
REFERENCES Kimberline, DW. Management of HSV Encephalitis in Adults and Neonates: Diagnosis, Prognosis, and treatment. Herpes. (14)1. 2007. Klein, R. “Clinical manifestations and diagnosis of herpes simplex virus type 1 infection”. UpToDate, version 17.2. Jan 2009. Klein, R. “Herpes Simplex Type 1 Encephalitis”. UpToDate, version 17.2. Feb 2009. Shandera, WX and H Koo. “Infectious Diseases: Viral & Rickettsial”. 2007 Current Medical Diagnosis & Treatment. 46th ed. The McGraw Hill Companies: USA. 2007.