Download
1 / 2
20 likes | 193 Vues
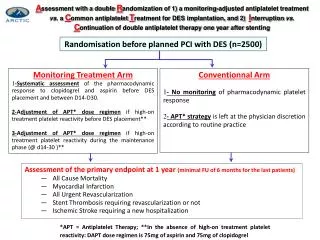
A ssessment with a double R andomization of 1) a monitoring-adjusted antiplatelet treatment vs. a C ommon antiplatelet T reatment for DES implantation, and 2) I nterruption vs. C ontinuation of double antiplatelet therapy one year after stenting.

E N D
Assessment with a double Randomization of 1) a monitoring-adjusted antiplatelet treatment vs. a Common antiplatelet Treatment for DES implantation, and 2) Interruption vs. Continuation of double antiplatelet therapy one year after stenting Randomisation beforeplanned PCI with DES (n=2500) • Monitoring Treatment Arm • -Systematicassessment of the pharmacodynamic response to clopidogrel and aspirinbefore DES placement and between D14-D30. • 2-Adjustment of APT* dose regimen if high-on treatmentplateletreactivitybefore DES placement** • 3-Adjustment of APT* dose regimen if high-on treatmentplateletreactivityduring the maintenance phase (@ d14-30 )** • Conventionnal Arm • - No monitoring of pharmacodynamic plateletresponse • - APT* strategyisleftat the physiciandiscretionaccording to routine practice • Assessment of the primary endpoint at 1 year (minimal FU of 6 months for the last patients) • All Cause Mortality • Myocardial Infarction • All Urgent Revascularization • Stent Thrombosis requiring revascularization or not • Ischemic Stroke requiring a new hospitalization *APT = Antiplatelet Therapy; **In the absence of high-on treatmentplateletreactivity: DAPT dose regimenis 75mg of aspirin and 75mg of clopidogrel
Planned PCI with DES, pretreated with aspirin and clopidogrel/prasugrel (local practice) and randomized to the Monitoring Treatment Arm VerifyNowbefore PCI : Aspirin & P2Y12 Thienopyridine %inh<15% /PRU>235 (P2Y12cartridge) ARU>550 (Aspirin cartridge) Reload with 500 mg of IV aspirin GPIIb/IIIainh. + clopidogrel (re)-loading (>or=600 mg) or prasugrel 60 mg and maintenance dose of 150 mg or prasugrel 10mg* VerifyNow @ day 14-30 Aspirin & P2Y12 thienopyridine for all patients • %inh>90% ARU>550 • %inh<15%/PRU>235 if clopidogrel 150mg, ↘ to 75mg or if on prasugrel switch to clopidogrel 75mg ↗Clopidogrel dose by at least 75 mg or switch to prasugrel 10mg* Doubling the aspirin dose * • Not indicatedif previous stroke. Caution in patients >75 yo or <60kg. • Indicated if Acute stent thrombosis or at least 2 of the followingriskfactors: • (i) diabetes or overweight(BMI>30); (ii) High on-treatmentplateletreacitivty; (iii) carriage of the 2C19*2 variant