Download
1 / 33
330 likes | 585 Vues
http://bahrain.cochrane.org http://www.rt.ae. Cochrane Collaboration and Systematic Review Workshop, 20-21 February 2007, Dubai - UAE. The Bahrain Branch of the UK Cochrane Centre In Collaboration with Reyada Training & Management Consultancy, Dubai-UAE. W03.

E N D
http://bahrain.cochrane.org http://www.rt.ae Cochrane Collaboration and Systematic Review Workshop, 20-21 February 2007, Dubai - UAE The Bahrain Branch of the UK Cochrane Centre In Collaboration with Reyada Training & Management Consultancy, Dubai-UAE W03 Dr. Zbys Fedorowicz, Dr. Dunia Al Hashimi, Dr. Ahmed Al Asfoor
Concepts to take home • Recognize types of studies • Recognize types of observational studies • Strengths and weaknesses of case-control and cohort study designs. • Recognize a controlled trial • Understand randomization, blinding/masking, placebos • Understand the ethics of clinical trials
Two Main Categories • Observational • Identify subjects first, then • Observe and record characteristics • Experimental • Identify subjects • Place in common context • Intervention, then • Observe effects of intervention
Types of studies • Observational studies • Case report/Case series • Case control • Cohort • Experimental studies
Basic Definitions • Retrospective - Any design that looks at data that have already been gathered • Prospective - Any design that collects data on groups of subjects over time, according to a carefully written protocol, beginning at time zero; this design yields data that enable comparisons of groups.
Basic Definitions • Bias - A methodological problem resulting from a selection process that is not random • Randomization - A process by which subjects are assigned to experimental or control groups so that the 2 groups are the same in all characteristics.
Basic Definitions • Population/target population - The total group of people who are represented by the random selection of members, usually connoting the whole population but possibly connoting the population of any subset, eg, women • Sample - A subset of subjects from the population of all who have a particular characteristic, such as a disease
Basic Definitions • Blinding - The process by which the identity of a subject's group assignment (case or control) is kept hidden from the subject • Double blinding - A process that ensures that both the subject and the caregiver or outcome assessor are unaware of whether the subject is assigned to the control or the experimental group.
Case control studies • Attempt to make inference from existing observations (retrospective) • Compares patients with outcome/disease with those without and attempts to identify factors that influenced that outcome (or caused that disease) • Important concept: start with the result (disease) and work backwards for the cause
Controls • A control is a standard of comparison for • Effects • Variability
Case-control studies • Controlled studies • Retrospective
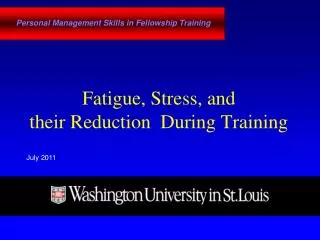
Case-control study design Exposure Disease Observer ? Choose groups with and without disease, look back at what different exposures they may have had
The logic of Case-Control Studies • Cases differ from controls only in having the disease. • If exposure does not predispose to having the disease, then exposure should be equally distributed between the cases and controls. • The extent of greater previous exposure among the cases reflects the increased risk that exposure confers
Strengths of case-control design • Best study when have rare disease or outcome • Relatively quick and inexpensive
Weaknesses (potential biases) • Selection (confounding) bias: controls must be as similar to cases as possible • Representativeness bias: cases should be “typical” • Recall bias: cases may be able to remember events better because of its significance or may be prompted to remember by investigators • Survival bias: dead people don’t make it into many case-cohort studies; and if they do, they don’t remember things very well
Cohort studies • Studies whether exposure to a “risk factor” is associated with a subsequent “outcome” • Select two populations who seem the same except for the hypothesized risk factor • Follow them ahead in time and see how many have the outcome or disease • Important concept: Start with the risk, then look for the outcome
Cohort studies • Prospective • Controlled • Can determine causes and incidence of diseases as well as identify risk factors • Generally expensive and difficult to carry out
Procedure for cohort study • Identify groups of exposed subjects and control subjects • Match for other risk factors • Follow over time • Record the fraction in each group who develop the condition of interest • Compare these fractions using RR or OR
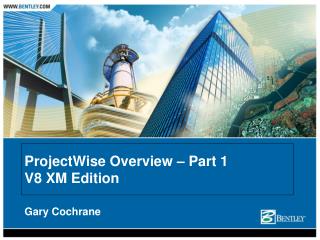
Logic of the cohort study Differences in the rate at which exposed and control subjects contract a disease is due to the differences in exposure, since other known risk factors are equally present in the two groups
Cohort study design (Prospective) Exposure Observer Disease ? Start with two groups of people who are exposed and unexposed, follow them to see who gets disease.
Strengths of cohort study • Not only can you look at risk, you can calculate how many people actually get the disease (incidence rates) • Since you enroll subjects before the outcome, you can measure multiple exposures without recall bias • Best for rare exposures
Potential biases in cohort studies • Selection (confounding) bias: have to match similar groups – “Healthy worker effect” • Detection bias: measurement of outcomes needs to be objective and similar for both groups • Length-time bias: study has to be long enough for outcome to happen • Excursion bias: subjects may disappear or drop-out (lost to follow-up)
Some other problems • Cohort studies may take a long time • Cohort studies may require a large number of people especially if the outcome is uncommon • Both of these make cohort studies expensive
Experimental design • Investigator controls exposure to the risk or treatment by assigning subjects to one group (experimental group) or another (control group) • Assignment to experimental or control attempts to make sure both group are similar in all ways except the experimental manipulation
Randomization of subjects • To help assure that groups are similar, subjects are randomly assigned to experimental or control groups • Randomization is performed to increase the likelihood that groups are matched in other, non-experimental ways • Randomization does not assure that the groups are the same: still need to assess whether they are
Randomised controlled trial (RCT) • Best form of healthcare evidence, or the “gold standard” for evidence about an intervention. • lack of randomisation can give a 40 % over or underestimate of treatment effect synthesis of those trials statistical and clinical heterogeneity.
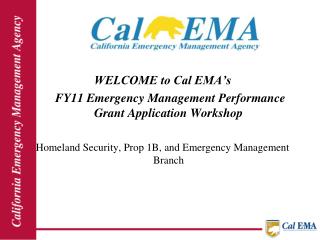
Randomised controlled trial intervention Outcome group 1 population Outcome group 2 control
RCT RCT SYSTEMATICREVIEW Meta-analysis RCT RCT “STRONGER” EVIDENCE
Randomization and Confounding • Randomization is supposed to have the effect of distributing confounders both known and unknown between the intervention and control groups
Blinding • Even after randomization, it is possible that experimental subjects may be treated differently than controls • To combat this, “blinding” is often used (also called masking) • Blinding means that the subject, investigator, or both (double-blind) do not know what group the subject is assigned to
Placebos • Placebos are another way of trying to make both groups similar • A placebo is a biologically inactive substance given to the control group so that they think they are being treated • “Placebo effect” is important: many patients in the placebo group report getting better simply because they are taking the placebo!
Are placebos ethical? • When there is no known successful therapy, a placebo is ethical (but withholding a treatment known to be effective is not!) • Using a placebo instead of the experimental drug is ethical since the experimental drug is not known to be beneficial and could actually be harmful