Download
1 / 21
210 likes | 214 Vues
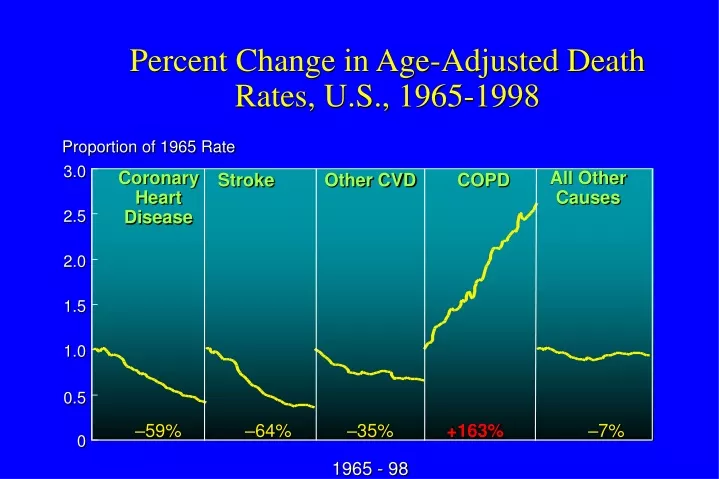
Percent Change in Age-Adjusted Death Rates, U.S., 1965-1998. Proportion of 1965 Rate. 3.0. Coronary Heart Disease. Stroke. Other CVD. COPD. All Other Causes. 2.5. 2.0. 1.5. 1.0. 0.5. –59%. –64%. –35%. +163%. –7%. 0. 1965 - 98. COPD - Pathogenesis. Tobacco Smoke.

E N D
Percent Change in Age-Adjusted Death Rates, U.S., 1965-1998 Proportion of 1965 Rate 3.0 Coronary Heart Disease Stroke Other CVD COPD All Other Causes 2.5 2.0 1.5 1.0 0.5 –59% –64% –35% +163% –7% 0 1965 - 98
COPD - Pathogenesis Tobacco Smoke Host factors Chronic Inflammation* Anti-oxidants Anti-proteinases Oxidative Stress Proteinases Repair Mechanisms Emphysema Chronic Bronchitis *CD8+ T-lymphocytes Macrophages Neutrophils IL-8 and TNF
Smoking Cessation Oxygen Reduce exacerbations Pulmonary Rehabilitation LVRS (selected patients) Lung Transplantation MDI Therapy SA beta-2 agonists LA beta-2 agonists SA and LA Anticholinergics Theophylline Corticosteroids (inhaled or oral) Combination Preparations SABA and anticholinergic LABA and corticosteroids COPD Therapy Prolong Life Symptomatic
Management of COPD Stage 0: At Risk Characteristics Recommended Treatment • Risk factors • Chronic symptoms - cough - sputum • No spirometric abnormalities • Adjust risk factors • Immunizations
Management of COPD Stage I: Mild COPD Characteristics Recommended Treatment • FEV1/FVC < 70 % • FEV1> 80 % predicted • With or without symptoms • Short-acting bronchodilator as needed
Management of COPD Stage II: Moderate COPD Characteristics Recommended Treatment • Treatment with one or more long-acting bronchodilators • Rehabilitation • FEV1/FVC < 70% • 50% < FEV1< 80% predicted • With or without symptoms
Management of COPD Stage III: Severe COPD Characteristics Recommended Treatment • Treatment with one or more long-acting bronchodilators • Rehabilitation • Inhaled glucocortico-steroids if repeated exacerbations (>3/year) • FEV1/FVC < 70% • 30% < FEV1 < 50% predicted • With or without symptoms
Management of COPD Stage IV: Very Severe COPD Characteristics Recommended Treatment • Treatment with one or more long-acting bronchodilators • Inhaled glucocorticosteroids if repeated exacerbations (>3/year) • Treatment of complications • Rehabilitation • Long-term oxygen therapy if respiratory failure • Consider surgical options • FEV1/FVC < 70% • FEV1 < 30% predicted or presence of respiratory failure or right heart failure
Bronchodilator Therapy Some General Principles • Inhaled therapy (with spacer) preferred • Long-acting preparations more convenient • Combined preparations improve effectiveness and decrease risk of side effects • Ipratroprium-albuterol • Fluticasone-salmeterol • Budesonide-formoterol • MDI almost always as effective as nebulizers (in equal doses)
Effectiveness of BronchodilatorTherapy? • FEV1 does not always correlate with symptoms • Concept of “dynamic hyperinflation” in COPD • Quality of life issues are important • Chronic fatigue • Depression • Physical immobility • Dyspnea
COPD - Surgical Options • Giant Bullous Disease • Consider bullectomy if see normal lung compression • Lung Volume Reduction Surgery* • FEV1 (<20% pred) plus diffuse emphysema or Dlco<20% pred = high risk of surgical death • Upper lobe emphysema and low exercise capacity = decreased mortality, increased exercise and QOL • Lung Transplantation • FEV1<25% predicted, younger patient • 3-5 year mortality 55% *NETT Research Group. N Eng J Med 348:2059, 2003
COPD Exacerbation Definition Elements Severity • Worsening dyspnea • Increased sputum purulence • Increase in sputum volume • Severe - all 3 elements • Moderate - 2 elements • Mild - 1 element plus: • URI in past 5 days • Fever without apparent cause • Increased wheezing or cough • Increase (+20%) of respiratory rate or heart rate Modified from Anthonisen et al. Ann Int Med 106:196, 1987
COPD Exacerbation Effects on Lung Function Decline • 109 pts (mean FEV1 = 1.0 L over 4 years • Frequent exacerbators: • faster decline in PEFR and FEV1 • more chronic symptoms (dyspnea, wheeze) • no differences in PaO2 or PaCO2 Infrequent Frequent • Conclusion: • Frequent exacerbations accelerate decline in lung function Donaldson et al. Thorax 57:847, 2002
COPD Exacerbation Chronic Inflammation Acute Inflammation Exacerbation Pathophysiology - Current Hypothesis Viral Infection 25% Unknown 20% Bacterial Infection 50% Air Pollution 5%
Therapy of COPD Exacerbation Guidelines Ann Int Med 134:595, 2001 http:/www.goldcopd.com
Therapy of COPD Exacerbation Guidelines Ann Int Med 134:595, 2001 http:/www.goldcopd.com
Therapy of COPD Exacerbation Guidelines Ann Int Med 134:595, 2001 http:/www.goldcopd.com
COPD Therapy - New Horizons • Newer anti-inflammatory agents • Matrix metalloproteinase inhibitors • Specific phosphodiesterase (PDE4) inhibitors • Cilomilast • Rofumilast • Piklanilast • Anabolic steroids • Repair agents • Retinoic acid • Long-acting anti-muscarinic agents • tiotropium
Tiotropium Specific M1 and M3 Muscarinic Blockade • 470 patients - stable COPD • 3 month, randomized, double blind, once daily tiotropium vs. placebo • Conclusions: • Increased FEV1 and FVC • No tachyphylaxis • Decreased rescue albuterol • Decreased wheezing, SOB • Dry mouth in 9.3% Casaburi et al. CHEST 118:1294, 2000
Tiatroprium Specific M1 and M3 Muscarinic Blockade • 1207 patients, double blind, randomized trial, • qd tiotropium vs. bid salmeterol vs. placebo • Conclusions: Tiotropium • Fewer exacerbations • Increased time to first exacerbation • Fewer admissions • Increased QOL Brusasco et al. Thorax 58:399:2003
Lung Volumes in Obstructive Disease Lung Volumes in Obstructive Disease TLC TLC Room to Room to Breathe Breathe TLC TLC FRC FRC Room to Room to Volume Volume Breathe Breathe FRC FRC RV RV RV RV Normal Normal COPD COPD