ETHICAL FRAMEWORK
ETHICAL FRAMEWORK. [ENTER FACILITATOR’S NAME AND CONTACT INFORMATION]. Developed by Troutman Sanders LLP Developed for the Virginia Department of Health Funded by Centers for Disease Control and Prevention. Toolkit Presentations Instructions for Use.

ETHICAL FRAMEWORK
E N D
Presentation Transcript
ETHICAL FRAMEWORK [ENTER FACILITATOR’S NAME AND CONTACT INFORMATION] Developed by Troutman Sanders LLP Developed for the Virginia Department of Health Funded by Centers for Disease Control and Prevention
Toolkit Presentations Instructions for Use • Toolkit Presentations are intended to be a companion to the HospitalImplementation Guide and should not be used in isolation. • The Presentations are intended to serve as a starting point for the facilitator. The facilitator should thoroughly review the Presentation prior to use in Implementation Team, CRAG or Subcommittee meetings and customize the Presentation to meet the unique needs of the meeting participants. • Pay particular to attention to the information provided in brackets ([ ]), which must be completed by the facilitator prior to use. • Included in the “Notes” section of each slide are the following types of information: • Slide Type, which indicates whether the slide is for information or discussion, serves as a placeholder, or is some combination thereof • Planning Guide Section(s), which will direct the facilitator to the corresponding sections of the Planning Guide and HospitalImplementation Guide for further information • Special Instructions, which provides directions for the facilitator to customize the slide for the intended audience • Speaker’s Notes, which provides more detailed information to supplement the material on the slide • Refer to the Hospital Implementation Guide for further guidance and helpful hints on effectively completing the process described in the Planning Guide.
CRAG Members • [Enter names and departments of each CRAG member]
Add slides from Altered Standards Overview and/or Chapter 1 presentation, as needed, to re-introduce the CRAG to the concept of altered standards and critical resource shortage response planning, especially if new members are involved.
Why Ethics? • Decisions during a CRSE involve complex, challenging ethical issues, including the allocation of scarce resources • An ethical framework will help ensure that the CRSRP and associated Protocols are developed in an ethical manner • Ideally, the application of an ethical framework will produce a CRSRP and Protocols that are accepted as ethically sound • While existing frameworks may be helpful, Planning Units should create their own framework which reflects their unique culture and values
Protocol Protocol Protocol Protocol Protocol Protocol Protocol Protocol Building the CRSRP Strong Foundation Education & Communication Ad Hoc Operational Infrastructure Ethical Framework
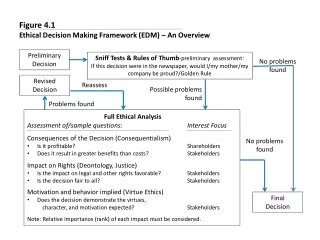
Three Step Process Step 1: Identify Ethical Principles Step 2: Define the Goal Step 3: Determine Implementation Specifications
Step 1: Identify Ethical Principles
Ethical Principles Substantive Principles • Individual Liberty • Protection of the public from harm • Proportionality • Distributive justice and fairness • Beneficence • Non-maleficence • Privacy • Duty to provide care • Reciprocity • Respect for Autonomy • Equity • Trust • Solidarity • Stewardship Procedural Principles • Reasonable • Open and Transparent • Inclusive • Responsive • Accountable
Substantive Individual Liberty Protection of the public from harm Proportionality Distributive justice and fairness Beneficence Non-maleficence Privacy Duty to provide care Reciprocity Respect for autonomy Equity Trust Solidarity Stewardship Procedural Reasonable Open and transparent Inclusive Responsive Accountable Prioritization of Ethical Principles High Low Medium
Potential Goals • Protecting the functionality of society • Protecting societal and community infrastructure • Preventing morbidity and mortality • Greatest good for the greatest number • Greatest good for the greatest number with “side constraints” • Greatest number of people benefited • Greatest number of lives saved • Greatest number of life years saved • Greatest number of quality life years saved
“Protecting the Functionality of Society” • Modify practices and allocate resources to protect the societal infrastructure and prevent it from breaking down under the stress of the disaster • Prioritize for prophylaxis and treatment those people who are essential to preserving the functionality of society • Who is essential to protecting the functioning of society? • Health care providers? • Public Health Officials? • Legislators? • Police officers? • Truck drivers? • Janitors? • Sewage workers? • Will the answer depend on the disaster or the type of care that is being modified or allocated?
“Prevent Morbidity and Mortality” • Modify practices and allocate resources to prevent illness and death • Prioritize for prophylaxis and treatment those people who are most likely to become ill, make others ill, or die without the intervention • Will the prioritization change based on the disaster or the type of care that is being modified or allocated?
“Greatest Good for Greatest Number” • Widely used in critical resource shortage response planning literature • Not clear exactly what it means • Greatest number of lives saved? • Greatest number of life years saved? • Greatest number of quality life years saved? • Greatest number of people benefited?
“Greatest Good for Greatest Number with Side Constraints” • Greatest good for the greatest number + Respect for persons + Non-maleficence + Justice • Greatest good for the greatest number + Refraining from harming individuals and communities + Providing equal opportunity to access resources to those in priority groups + Employing the least restrictive interventions likely to be effective
Choose a Goal • Protecting the functionality of society • Protecting societal and community infrastructure • Preventing morbidity and morality • Greatest good for the greatest number • Greatest good for the greatest number with “side constraints” • Greatest number of people benefited • Greatest number of lives saved • Greatest number of life years saved • Greatest number of quality life years saved
Withdrawal and Reallocation • Will providers be allowed to withdraw resources from one patient to give them to another patient? • If so, under what general circumstances?
Consider that… • If you are not willing to withdraw treatment, then you are essentially providing care on a first come, first served basis. • If you are willing to withdraw care, will this be construed as valuing one person’s life more than another’s life?
Withholding of Resources • Will providers be allowed to withhold a critical resource from one patient to conserve it for a future patient? • If so, under what general circumstances? • Is the answer different for durable v. consumable resources?
Consider that … • If you are not willing to withhold care, you will essentially be providing care on a first come, first served basis. • If you are willing to withhold care, you may have unused, available resources that are not being provided to a patient in need.
“Inclusion” and “Exclusion” Criteria • Many of the existing allocation algorithms include “inclusion” and “exclusion” criteria Inclusion Criteria Those patient characteristics which indicate a need for the Critical Resource Exclusion Criteria Those patient characteristics that remove a patient from consideration for the Critical Resource even when the inclusion criteria are met
Example Exclusion CriteriaOntario Health Plan for Influenza Pandemic Christian MD, et al. (Nov 2006) “Development of a Triage Protocol for Critical Care During an Influenza Pandemic.” CMAJ, 175(11): 1377-1381. Available online at: http://www.cmaj.ca/cgi/reprint/175/11/1377 (last visited March 9, 2009).
Example Exclusion CriteriaNew York Vent Allocation Guidance Powell T, et al. (Mar 2008) “Allocation of Ventilators in a Public Health Disaster.” Disaster Medicine and Public Health Preparedness, 2(1): 20-26.
Example Exclusion CriteriaTask Force for Mass Critical Care Working Group Devereaux A, et al. (2008) “Definitive Care for the Critically Ill During a Disaster: A Framework for Allocation of Scarce Resources in Mass Critical Care.” Chest, 133: 51S-66S. Available online at:http://www.chestjournal.org/content/133/5_suppl/51S.full (last visited March 9, 2009).
Example Exclusion CriteriaUtah Pan Flu Hospital and ICU Triage Utah Department of Health (Aug 2008) “Utah Pandemic Influenza Hospital and ICU Triage Guidelines.” http://www.uha-utah.org/Disaster%20Prep%20Materials/PANDEMIC%20FLU%20TRIAGE%2008-12-08.pdf (last visited March 9, 2009).
CA’s Exclusion Criteria Guidance Acceptable • Likelihood of survival • Change in quality of life • Duration of benefit • Urgency of need • Amount of resources required Inappropriate • Ability to pay • Social worth • Patient contribution to disease • Past use of resources California Department of Public Health. (2007). “California Department of Public Health Standards and Guidelines for Healthcare Surge During Emergencies, Volume I: Hospitals.” Available online at:http://bepreparedcalifornia.ca.gov/NR/rdonlyres/0DB13C5F-89DC-4B94-850B-EF12EA221FF3/0/volume1_hospital_FINAL.pdf (last visited September 25, 2009).
Ability to pay? Social worth? Race or ethnicity? Religion? Gender? Patient contribution to disease? Past use of resources? Age? If so, what is the cut-off? Severe baseline cognitive impairment? Known severe dementia? Metastatic malignant disease? End stage organ failure? Severe and irreversible neurological event or condition? Advanced and irreversible immunocompromise? Advanced untreatable neuromuscular disease? Known chromosomal or untreatable disorders fatal in first 2 years of life? Inappropriate Exclusion Criteria

![[Report] The Trust Imperative: A Framework for Ethical Data Use](https://cdn4.slideserve.com/7526233/preview-only-dt.jpg)