RETROVIRUSES
RETROVIRUSES. Virology lectures Inass Aziz Malik. Retroviridae. This large and diverse family includes members that are oncogenic, are associated with a variety of immune system disorders, and cause degenerative and neurological syndromes. Natural host.

RETROVIRUSES
E N D
Presentation Transcript
RETROVIRUSES Virology lectures Inass Aziz Malik
Retroviridae • This large and diverse family includes members that are oncogenic, are associated with a variety of immune system disorders, and cause degenerative and neurological syndromes.
Natural host • Natural host range is limited to human, certain primates can be infected (lab) • Chimpanzees in west Africa are the source of HIV-1 (evidence)
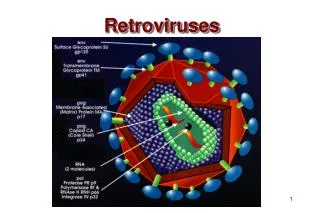
Single stranded (+) RNA viruses, enveloped viruses RNA-dependent-DNA Polymerase (Reverse transcriptase). This enzyme converts the RNA genome into DNA, which then integrates into the host chromosomal DNA. The reverse transcriptase is highly error prone and rapid genetic variation (during the course of disease) is a feature of this group.
Human Immunodeficiency Virus AIDS first described in 1981 • HIV-1 isolated in 1984, and HIV-2 in 1986 • Belong to the lentivirus subfamily • Enveloped RNA virus, 80-120nm in diameter • HIV-2 shares 40% nucleotide homology with HIV-1
Genome organization The virus has a diploid genome (2 copies of RNA genome per virus particle). The genome codes for at least three genes: gag, pol and env: gag - codes for the core proteins, structural virion components pol - reverse transcriptase env - envelope glycoprotein
gag, pol, and env 1/ Gag protein proteolytically processed into: • MA (matrix) • CA (capsid) • NC (nucleocapsid)
Retrovrius proteins 2/ Pol protein encodes enzymes: • PR (protease) • RT (Reverse Transcriptase which has both DNA polymerase and RNase H activities) • IN (Integrase)
Retrovirus protein 3/ Env protein encodes: • SU surface glycoprotein • TM transmembrane protein
Env Proteins: Surface (SU) • Glycoprotein , attaches to a specific receptor on cell surface • Major neutralizing antigen on retrovirus, also often highly variable (EIAV, HIV). Hard to make vaccines. SU (gp120) Lipid Bilayer (derived from cell) TM (gp 41)
“Accessory” genes (in Complex Retroviruses) - regulate and coordinate virus expression; function in immune escape • Oncogene products (v-Onc, in Acutely Transforming Retroviruses) - produce transformed phenotype
HIV accessory proteins Vif Protein: • Viral infectivity factor • Accumulates in the cytoplasm and at the plasma membrane of infected cells • Mutant viruses lacking the vif gene were less infectious and defective in some way (primates) • vif-defective virions enter cells, initiate reverse transcription, but do not produce full-length double stranded DNA
Replication • The first step of infection is the binding of gp120 to the CD4 receptor of the cell, which is followed by penetration and uncoating (fusion or endocytosis in other retroviruses). • The RNA genome is then reverse transcribed into a DNA provirus which is integrated into the cell genome.
Retrovirus replication cycle • Transit of the DNA to the nucleus • Integration of the viral DNA into random sites in cellular DNA to form the provirus • Synthesis of viral RNA by cellular RNA polymerase II using the integrated provirus as a template • Processing of the transcripts to genome and mRNAs • Synthesis of virion proteins • Assembly and budding of virions • Proteolytic processing of capsid proteins
HIV binding and entry •The gp120 has a specific domain that binds to the CD4 molecule present on susceptible cells •Upon binding to CD4, the gp120 undergoes a conformational change that allows binding to specific subset of chemokine receptors on the cell surface, the CCr5 receptor and the CXCr4 receptor
Transmission of the virus • Transfer of HIV infected cells • Free HIV • No evidence of saliva and tears transmission • Much less efficiently transferred than HBV (dose dependent) • Infectious dose is high
HIV enters the bloodstream through: Open Cuts Breaks in the skin Mucous membranes Direct injection HIV Transmission
Common fluids that are a means of transmission: Blood Semen Vaginal Secretions Breast Milk HIV Transmission
Routes of Transmission of HIV Sexual Contact:Male-to-male Male-to-female or vice versa Female-to-female Blood Exposure:Injecting drug use/needle sharing Occupational exposure Transfusion of blood products Perinatal:Transmission from mom to baby Breastfeeding
Window Period • This is the period of time after becoming infected when an HIV test is negative • 90 percent of cases test positive within three months of exposure • 10 percent of cases test positive within three to six months of exposure
HIV Infection and Antibody Response ---Initial Stage---- ---------------Intermediate or Latent Stage-------------- ---Illness Stage--- Flu-like Symptoms Or No Symptoms Symptom-free AIDS Symptoms ---- Infection Occurs ---- <
Clinical Features 1. Seroconversion illness - seen in 10% of individuals a few weeks after exposure and coincides with seroconversion. Presents with an infectious mononucleosis like illness.
2. Incubation period - this is the period when the patient is completely asymptomatic and may vary from a few months to a more than 10 years. The median incubation period is 8-10 years. 3. AIDS-related complex or persistent generalized lymphadenopathy. 4. Full-blown AIDS.
Opportunistic Infections Protozoal: toxoplasmosis, crytosporidosis Fungal: pneumocystis carinii candidiasis, crytococcosis histoplasmosis, coccidiodomycosis
Bacterial: • Mycobacterium avium complex, MTB • atypical mycobacterial disease • salmonella septicaemia • multiple or recurrent pyogenic bacterial infection Viral : CMV, HSV, VZV
Opportunistic Tumours • The most frequent opportunistic tumour, Kaposi's sarcoma, is observed in 20% of patients with AIDS. • KS is observed mostly in homosexuals and its relative incidence is declining. It is now associated with a human herpes virus 8 (HHV-8). • Malignant lymphomas are also frequently seen in AIDS patients.
HIV Pathogenesis • The profound immunosuppression seen in AIDS is due to the depletion of T4 helper lymphocytes. • In the immediate period following exposure, HIV is present at a high level in the blood (as detected by HIV Antigen and HIV-RNA assays).
It then settles down to a certain low level (set-point) during the incubation period, there is a massive turnover of CD4 cells, whereby CD4 cells killed by HIV are replaced efficiently. • Eventually, the immune system succumbs and AIDS develop when killed CD4 cells can no longer be replaced (witnessed by high HIV-RNA, HIV-antigen, and low CD4 counts).
Laboratory Diagnosis • Serology is the usual method for diagnosing HIV infection. Serological tests can be divided into screening and confirmatory assays. Screening assays should be as sensitive whereas confirmatory assays should be as specific as possible. • Screening assays - EIAs are the most frequently used screening assays. The sensitivity and specificity of the presently available commercial systems now approaches 100% but false positive and negative reactions occur. Some assays have problems in detecting HIV-1 subtype O.
Confirmatory assays - Western blot is regarded as the gold standard for serological diagnosis. However, its sensitivity is lower than screening EIAs. Line immunoassays incorporate various HIV antigens on nitrocellulose strips. The interpretation of results is similar to Western blot it is more sensitive and specific.
Treatment HAART (Highly active antiretroviral therapy) • Two nucleoside inhibitors (Zidovudine and Lamivudine) • and a protease inhibitor (Indinavir)