Download
1 / 68
680 likes | 791 Vues
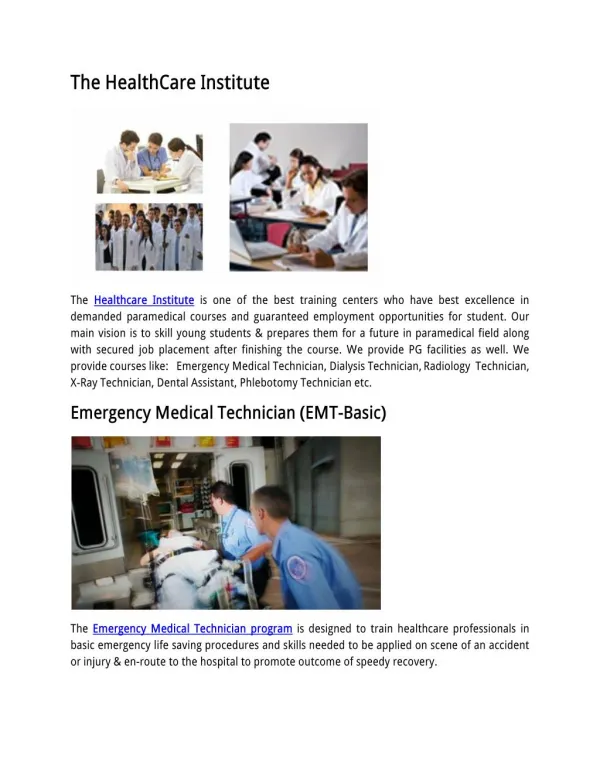
Wednesday, May 2, 2012 Hilton New York 1335 Avenue of the Americas New York, New York. Premier Healthcare Training Institute . James (Larry) Holly, MD CEO, SETMA, LLP www.setma.com Adjunct Professor Department of Family and Community Health School of Medicine

E N D
Wednesday, May 2, 2012 Hilton New York 1335 Avenue of the Americas New York, New York Premier Healthcare Training Institute
James (Larry) Holly, MD CEO, SETMA, LLP www.setma.com Adjunct Professor Department of Family and Community Health School of Medicine The University of Texas Health Science Center at San Antonio Large-scale Medical Management of Patients Using Quality Indicators and Electronic Health Records
If health science has the capacity: • To create far more information than anyone can absorb, • To foster far greater interdependency than anyone can manage, • To accelerate change far faster than anyone’s ability to keep pace.
EMR Power How can electronic patient records and/or electronic patient management help solve these problems and make it possible for healthcare providers to remain current and fulfill their responsibility of caring for patients with the best treatments available?
Data flow to and from the patient’s core information, and to and from interactive disease management capabilities: • Acute condition data • Longitudinal data • Standards of care which reflect a positive state of health • Automatically-populated-treatment reflecting best practices based on random controlled trials • Auditing tools which reflect provider excellence • Automatically-populated-patient follow-up instructions • Automatically-created-patient education
Forward Thinkers Have Personal Mastery • Personal Mastery – the discipline of continually clarifying and deepening our personal vision, of focusing our energies, of developing patience, and of seeing reality objectively – the learning organization’s spiritual foundation. (Peter Senge) • “The essence of personal mastery is learning how to generate and sustain creative tension in our lives.”
Personal Mastery: Characteristics People with a high level of personal mastery share several basic characteristics: • The have a special sense of purpose that lies behind their vision and goals. For such a person, a vision is a calling rather than simply a good idea. • They see current reality as an ally, not an enemy. They have learned how to perceive and work with forces of change rather than resist those forces.
Personal Mastery: Characteristics • They are deeply inquisitive, committed to continually seeing reality more and more accurately. • They feel connected to others and to life itself. • Yet, they sacrifice none of their uniqueness. • They feel as if they are part of a larger creative process, which they can influence but cannot unilaterally control. (p. 142)
Personal Mastery: Characteristics • Live in a continual learning mode. • They never ARRIVE! • (They) are acutely aware of their ignorance, their incompetence, their growth areas. • And they are deeply self-confident!
Trust and Hope In the midst of health information technology innovation, we must never forget that the foundations of healthcare change are “trust” and “hope.” Without these, science is helpless!
Domains of Healthcare Transformation • The Substance -- Evidenced-based medicine and comprehensive health promotion • The Method -- Electronic Patient Management • The Organization -- Patient-centered Medical Home • The Funding -- Capitation with payment for quality outcomes
The SETMA Model of Care The SETMA Model of Care is comprised of five critical steps: • Tracking • Auditing • Analyzing • Public Reporting • Quality Improvement
Clusters and Galaxies SETMA believes that fulfilling a single or a few quality metrics does not change outcomes, but fulfilling “clusters” and “galaxies” of metrics at the point-of-care will change outcomes. • A “cluster” is seven or more quality metrics for a single condition (i.e. diabetes, hypertension, etc.) • A “galaxy” is multiple clusters for the same patient (i.e. diabetes, hypertension, lipids, CHF, etc.)
A Cluster A single patient, at a single visit, for a single condition, will have eight or more quality metrics fulfilled, which WILL change the outcome of a patient’s treatment.
A Galaxy A single patient, at a single visit, can have multiple clusters of quality metrics and may have as many as 60 or more quality metrics fulfilled in his/her care which WILL change the outcomes.
The SETMA Model of Care SETMA’s model of care is based on the concepts of “clusters” and “galaxies” of quality metrics and on these principles of healthcare transformation: • Evidence based medicine/health and wellness • Electronic patient management • Patient-Centered Medical Home • Medicare Advantage Payment Method (capitation)
Step 1 –Tracking Quality Metrics The tracking on each patient by each provider of their performance on preventive and screening care and quality standards for acute and chronic care. Tracking occurs simultaneously with the performing of these services by the entire healthcare team, including the personal provider, nurse, clerk, management, etc.
Step 1 –Tracking Quality Metrics • The PCPI is an organization created by the AMA, CMS, IOM and others to develop measurement sets for quality-care assessment. The intent is to allow healthcare providers to evaluate their own performance at the time they are seeing a patient. • SETMA tracks PCPI measurement sets for Chronic Stable Angina, CHF, Diabetes, Hypertension, and CRD Stages IV & V, ESRD, Adult Weight Management, and Care Transitions.
Step 1 –Tracking Quality Metrics • SETMA also tracks measurement sets endorsed by NQF. NCQA (HEDIS and Medical Home), PQRS, AQA, Guidelines Advantage Medicare Advantage STARs, Meaningful Use and Bridges to Excellence. Also, SETMA designed a Pre-visit quality measures screening and preventive care tool. • Where quality metrics did not exist (Lipids, Stage I-III Renal disease) SETMA designed our own. • This allows a SETMA provider and a patient to quickly and easily assess whether or not the patient has received all of the appropriate preventive health care and the appropriate screening health care which national standards establish as being needed by this patient.
Step 1 –Tracking Quality Metrics Pre-Visit Preventive/Screening tool • All measures in black apply to the current patient and are fulfilled. • All measures in red apply to the current patient and have not been fulfilled. • All measures in grey do not apply to the current patient. If a point of care is missing, it can be fulfilled with the single click of a single button.
Step 1 –Tracking Quality Metrics There are similar tracking tools for all of the quality metrics which SETMA providers track each day. Such as this example of NQF-endorsed measures.
Step 1 –Tracking Quality Metrics In order for the tracking of quality metrics to be valuable to the patient, the patient must know what is being tracked, what it means and what has or has not been performed in his/her own care.
Passing the Baton • If responsibility for a patient’s healthcare is symbolized by a baton, the healthcare provider carries the baton for .68% of the time. The patient carries the baton 99.22% of the time. • Coordination of care between healthcare providers is important but the coordination of the patient’s care between the healthcare provider and the patient is imperative.
Passing the Baton “Often, it is forgotten that the member of the healthcare delivery team who carries the ‘baton’ for the majority of the time is the patient and/or the family member who is the principal caregiver. If the ‘baton’ is not effectively transferred to the patient or caregiver, the patient’s care will suffer.” SETMA
The Baton – What Does it Mean? In all public areas and in every examination room, SETMA’s “Baton” poster is displayed. It illustrates: • That the healthcare-team relationship, which exists between patient and healthcare provider, is key to the success of the outcome of quality healthcare. • That the plan of care and treatment plan, the “baton,” is the engine through which the knowledge and power of the healthcare team is transmitted and sustained.
The Baton – What Does it Mean? • That the means of transfer of the “baton”, which has been developed by the healthcare team is a coordinated effort between the provider and the patient. • That typically the healthcare provider knows and understands the patient’s healthcare plan of care and the treatment plan, but without its transfer to the patient, the provider’s knowledge is useless to the patient. • That the imperative for the plan – the “baton” – is that it be transferred from the provider to the patient, if change in the life of the patient is going to make a difference in the patient’s health.
The Baton – What Does it Mean? • That this transfer requires that the patient “grasps” the “baton,” i.e., that the patient accepts, receives , understands and comprehends the plan, and that the patient is equipped and empowered to carry out the plan successfully. • That the patient knows that of the 8,760 hours in the year, he/she will be responsible for “carrying the baton,” longer and better than any other member of the healthcare team.
The Baton – What Does it Mean? • There are numerous points of “care transition” in the patient's care. In the transition of care from the hospital, there are potential eight different types of care transition. • PCPI has published a “Transition of Care Measurement Set,” which is illustrated here.
Transition of Care Measurement • The second, third and fourth of the transitions of care involve “follow-up call” scheduling: • The day following discharge from the hospital – this goes to follow-up call nursing staff in our Care Coordination Department. These calls differ from the “administrative calls’ initiated by the hospital which may last for 30 seconds are less. These calls last from 12-30 minutes and involved detailed discussions of patient’s needs and conditions.
Step 2 – Auditing Provider Performance • The auditing of provider performance on the entire practice, on each individual clinic, on each provider on a population, or on each provider on a panel of patients is critical for quality improvement. SETMA believes that this is the piece missing from most healthcare improvement programs.
Step 2 – Auditing Provider Performance • The creating of quality measures is a complex process. That Is why it is important for agencies such as the AQA, NCQA, NQF, PQRS and PCPI, among others, to identify, endorse and publish quality metrics. • The provider’s ability to monitor their own performance and the making of those monitoring results available to the patient is important, but it only allows the provider to know how they have performed on one patient.
Step 2 – Auditing Provider Performance • The aggregation of provider performance results over’ his/her entire panel of patients carries the process of designing the future of healthcare delivery a further and a critical step. • Most auditing results, such as HEDIS, are presented to the provider 12 to 18 months after the fact. SETMA believes that “real time, auditing and giving of the audit results to providers can change provider behavior and can overcome “treatment inertia.”
Step 2 – Auditing Provider Performance • Auditing of provider performance allows physicians and nurse practitioners to know how they are doing in the care of all of their patients. • It allows them to know how they are doing in relationship to their colleagues in their clinic or organization, and also how they are performing in relationship to similar practices and providers around the country.
Step 2 – Auditing Provider Performance • SETMA designed auditing tools through a Business intelligence software. (see SETMA’s BI Project at www.setma.com under Your Life Your Health and the icon COGNOS.) • Through BI Audits, SETMA is able to display outcomes trending which can show seasonal patterns of care and trending comparing one provider with another.
Step 2 – Auditing Provider Performance • It is also possible to look at differences between the care of patients who are treated to goal and those who are not. • Patients can be compared as to socio-economic characteristics, ethnicity, frequency of evaluation by visits and by laboratory analysis, numbers of medication, payer class, cultural, financial and other barriers to care, gender and other differences. This analysis can suggest ways in which to modify care in order to get all patients to goal.
Step 2 – Auditing Provider Performance • Using digital dashboard technology, SETMA analysis provider and practice performance in order to find patterns which can result in improved outcomes practice wide for an entire population of patients. We analyze patient populations by: • Provider Panel • Practice Panel • Financial Class – payer • Ethic Group • Socio-economic groups
Step 2 – Auditing Provider Performance • We are able to analyze if there are patterns to explain why one population or one patient is not to goal and others are. WE can look at: • Frequency of visits • Frequency of testing • Number of medications • Change in treatment • Education or not • Many other metrics