Download
1 / 2
1.11k likes | 2.31k Vues
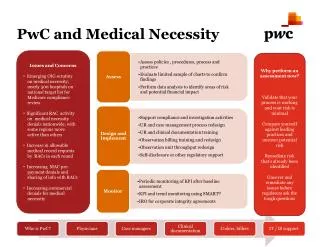
PwC and Medical Necessity. Issues and Concerns Emerging OIG scrutiny on medical necessity; nearly 500 hospitals on national target list for Medicare compliance review Significant RAC activity on medical necessity denials nationwide, with

E N D
PwC and Medical Necessity • Issues and Concerns • Emerging OIG scrutiny • on medical necessity; • nearly 500 hospitals on • national target list for • Medicare compliance • review • Significant RAC activity • on medical necessity • denials nationwide, with • some regions more • active than others • Increase in allowable • medical record requests • by RACs in each round • Increasing MAC pre- • payment denials and • sharing of info with RACs • Increasing commercial • denials for medical • necessity Why perform an assessment now? Validate that your process is working and your risk is minimal Compare yourself against leading practices and uncover potential risk Remediate risk that’s already been identified Uncover and remediate any issues before regulators ask the tough questions
Inactive or underutilized utilization review function Policy to admit when in doubt and determine retrospectively Confusing or missing physician orders Lack of standard admissions criteria and tools No customization of tools Misuse of tools used to assess medical necessity Over-ride of screening tools, without supporting documentation Lack of consistent admission practices and processes No ability to admit outpatients to units Missing or incomplete documentation of real factors used to make patient status decision Missing or incomplete documentation of actual observation activities during stay Determination of patient status made in billing (e.g., was in bed, so it’s inpatient) Lack of controls or monitoring in place; no update process Case management coverage at points of entry or vacation/weekend backup plan Common Pitfalls – Decision to admit Billing • Inappropriate use of condition code 44 • Over use - after patient leaves or defaulting to admission • Under use - not using condition code 44 • Failure to document MD consensus on status change • Calculation of observation hours: • Begins: when observation services start • Ends: with physician discharge order • Stays greater than 48 hours • Coding errors • Systems interfaces: generating a clean OBS bill, particularly after using conditioncode 44 For more information, please contact: Ann Filiault, director, (518) 427-4501 Laurie Smaldon, manager, (860) 241-7011 Ann Edwards, managing director, (617) 530-7634 Sandy Fortney, RN, manager, (267) 330-2592 Deedie Root, RN, managing director, (713) 356-8532 Advisory Proposal •