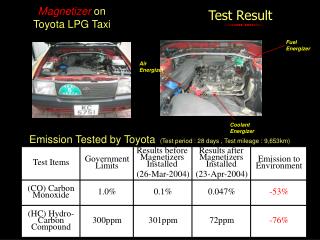
Result
RANKL/OPG serum concentration ratio as a new biomarker for coronary artery calcification Amir Hooshang Mohammad pour 1 , Saeed Nazemi 2 , Mohammad Ramezani 3 , Samira Ghadirzadeh 3 , Shabnam Shahsavand 4 , Hayedeh Hashemizadeh 5 , Negar Milani Moghadam 4

Result
E N D
Presentation Transcript
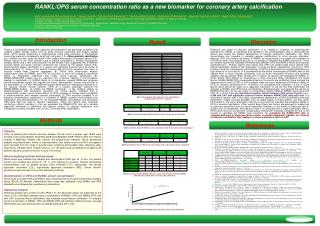
RANKL/OPG serum concentration ratio as a new biomarker for coronary artery calcification Amir Hooshang Mohammad pour1, Saeed Nazemi2, Mohammad Ramezani 3 , Samira Ghadirzadeh3, Shabnam Shahsavand4 , Hayedeh Hashemizadeh5 ,NegarMilani Moghadam4 1:Pharmaceutical research center and school of pharmacy , Department of Pharmacodinamy and Toxicology, Mashhad University of Medical Sciences 2.Razavi hospital , cardiovascular department 3. Pharmaceutical research center and school of pharmacy , Department of Biotechnology, Mashhad University of Medical Sciences 4. School of pharmacy, Mashhad University of Medical Sciences 5.Ghuchan Azad University Introduction Result Discusion There is a considerable demand for diagnosis and treatment of the pathologic conditions that underlie sudden cardiac events such as acute coronary syndromes and sudden cardiac death. Some people experience a cardiovascular event while according to Framingham scores they were not considered to be at high risk group (1,2). Atherosclerotic calcification is a condition that can make the break in the vessels and causes the plaque rupture (3,4). Plaque rupture is the most common type of plaque complications. Several retrospective autopsy series and a few cross-sectional clinical studies have suggested that thrombotic coronary death and acute coronary syndromes are caused by the plaque rupture (5,6). Atherosclerotic plaque calcification is a regular and organized process that is so similar to osteoproduction (7). Some of the smooth muscle cells during the migration from layer to vascular media layer, become osteogenic (8). These cells continuously express osteoproteins such as RANKL and OPG (4) and start to store the collagenic extrcellular metrix in mineralized collections that finally cause vascular calcification (9). RANKL/RANK/OPG system has an important role in several aspects of the processes leading to calcification (3) RANKL Binds to its membrane receptor-RANK-and produces several intracellular signals that regulate the fusion, development, function and survival of the osteoclasts (2, 3) It also stimulates the gradual development of osteogenic calcification in the vascular smooth muscle cells(10). OPG as a soluble scavenger presents the RANKL/RANK binding so inhibits the RANKL function(3). It has inhibitory effects on osteoclastogenes and osteogenic resorbtion (2). Some reports indicated that in cardiovascular system, serum concentration of OPG increases in clinical cases susceptible to atheroschlerosis and unstable vascular calcification (3) OPG secretion probably is an imperfect compensatory mechanism v.s increment of RANKL secretion that prevents over calcification and atheroschlerosis (11). So increased RANKL concentration and decreased OPG level both can lead to vascular calcification. These two factors have reciprocal (conflicting) effects. Acording to this we evaluated the RANKL/OPG ratio as a suitable diagnostic biomarker to determine the intensity (extent) of vascular calcification and subsequent coronary disorders such as CAC (Coronary Artery calcification). Presence and extent of vascular calcification is so related to incidence of cardiovascular disorders(11). RANKL is expressed and secreted in the semisteoblastic cells in atherosclerotic lesions and causes the gradual development of vascular osteogenic calcification (12). OPG concentration also increase in unstable vascular calcifications or other vascular disorders. Although OPG can prevent the effects of RANKL by antagonizing it but maybe the increment in OPG serum level, as a protective factor, is not enough to neutralize the RANKL effects(13). There are several reports that indicated the relationship between OPG and RANKL effects and vascular calcification(14 ). Primary reports have shown that OPG can protect large blood vessels from arterial calcification based on the observation of renal and aortic calcifications occurring in OPG knockout mice(15). Intravascular administration of OPG could prevent the induced calcification by high dosed of vit D in rats(16). It is considered that the serum concentration of RANKL were in the highest level in acute vascular syndromes such as acute myocardial infraction and ischemic cerebral vascular attacks (Brain strokes)(17). It seems, all reports just evaluated the RANKL or OPG, almost OPG effects on development of CAC (Coronary Artery calcification) but these factors, RANKL/RANK/OPG, have related effects so the results are conflicting. Some included the increase serum level of OPG in CAC however there are some evidences of inhibitory effects of OPG on vascular calcification(18 ). Therefore it is considered that evaluation of any of these factors alone cannot be useful as a diagnostic biomarker so we the first time determined the changes in RANKL and OPG levels contemporary (Simultaneously) and reported the results as RANKL/OPG ratio. As we see, there is no significant relation between RANKL serum level and CAC (P= 0.2) but there are significant negative relation between OPG serum (P=0.03, c.c= -0.468 and CAC and significant positive relation between RANKL/OPG ratio with that. It is important to mention that, in this study, measurement (deliberation) of OPG and RANKL level was performed in stable coronary disorders such as stable angina. In these patients, the less serum OPG levels is, the more calcification intensity is occurred, this indicates the protective effects of OPG in vascular calcification. Other reports about these two factors are belonged to researches on coronary syndromes such as acute myocardial infraction, so the results of these two type of studies are not comparable. According to these it is concluded that in urgent pathologic events, OPG serum level as a preventive compensatory mechanism markedly increased but this is not enough to neutralize the RANKL level increment. So evaluating the RANKl/OPG ratio in compare with each of these two factors alone, is a better diagnostic indicator for intensity of vascular calcification that leading to coronary disorders such as CAC. Table 1: Demographic data, Laboratory tests and traditional cardiovascular risk factors of patients Table2: Correlation between RANKL:OPG ratio with coronary artery calcification Methods References Table3:Correlation between RANKL serum concentration with total coronary artery calcification Patients Forty six patients with ischemic coronary disease (33 men and 13 women, age 18-60) were enrolled in this study between November 2008 and September 2009. Patients were from Razavi hospital in Mashhad. Patients with calcium and phosphorous metabolic failure, parathyroid disease, renal dysfunction, history of osteodisorders, Zero calcium score and Vit D consupation were excluded from the study. A questionnaire containing demographic data, laboratory data, drug history, medical history, familial history of C.V. risk factors was completed for all patients. All patients signed a consent form prior to entry in the study. Blood sampling and biochemical assay Whole blood was isolated from patients and centrifuged at 2500 rpm for 10 min. The plasma fraction was isolated and stored at -70°C until required for analysis. Routine biochemical measurements such as plasma glucose, total cholesterol (TC), triglycerides, low density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), Serum calcium, phosphorus were carried out by routine laboratory methods. Determination of OPG and RANKL serum concentration Serum level of soluble OPG and RANKL were measured with an enzyme-linked immunosorbant assay (ELIZA) kit (Apotech, Switzerland) each assay was calibrated using RANKL and OPG standard curve following the manufacture’s instructions. Statistical analysis Statistical analysis was carried out with SPSS 11.5. All measured values are presented as the mean ± SD. Correlation between serum concentration of RANKL ,OPG and RANKL/OPG ratio with CAC (Coronary Artery calcification) was analyzed using Pearson correlation. To compare serum concentration of RANKL ,OPG and RANKL/OPG ratio between different groups, one-way ANOVA test was used. Results were considered significant at P< 0.05. Abedin, M., Omland, T. Ueland, T. Khera, A. Aukrust, P. Murphy, S.A. Jain, T. Gruntmanis, U. McGuire, D.K. and de Lemos, J.A..(2007).Relation of osteoprotegerin to coronary calcium and aortic plaque (from the Dallas Heart Study). Am J Cardiol .,99 , 513-518. Abedin, M., Tintut, Y. And Demer, L.L.( 2004). Vascular calcification: mechanisms and clinical ramifications. Arterioscler Thromb Vasc Biol.,24 , 1161-1170. Anand, D.V., Lahiri, A. Lim, E. Hopkins, D. and Corder, R..(2006).The relationship between plasma osteoprotegerin levels and coronary artery calcification in uncomplicated type 2 diabetic subjects. J Am Coll Cardiol., 47 , 1850-1857. Asanuma, Y., Chung, C.P., Oeser, A., Solus, J.F., Avalos, I., Gebretsadik, T., Shintani, A., Raggi, P., Sokka, T., Pincus, T. and Stein, C.M..(2007). Serum osteoprotegerin is increased and independently associated with coronary-artery atherosclerosis in patients with rheumatoid arthritis. Atherosclerosis .,195,e135-e141 Boyce, B.F. and Xing, L.(2007). Biology of RANK, RANKL, and osteoprotegerin. Arthritis Res Ther.,9 , Suppl 1:S1. Budoff, M.J., Achenbach, S. Blumenthal, R.S., Carr, J.J., Goldin, J.G., Greenland, P. Guerci, A.D., Lima, J.A.C., Rader, D.J., Rubin, G.D., Shaw, L.J. and Wiegers, S.E..(2006). Assessment of Coronary Artery Disease by Cardiac Computed Tomography. Circulation ., 114 , 1761-1791. Collin-Osdoby, P..(2004). Regulation of vascular calcification by osteoclast regulatory factors RANKL and osteoprotegerin. Circ Res.,95 ,1046-1057. Crisafulli, A., Micari, A., Altavilla, D., Saporito, F., Sardella, A.,Passaniti, M., Raffa, S., D'Anneo, G., Luca, F., Mioni, C., Arrigo, F. and Squadrito, F..(2005).Serum levels of osteoprotegerin and RANKL in patients with ST elevation acute myocardial infarction. Clin Sci (Lond)., 109 , 389-395. Doherty, T.M., Fitzpatrick, L.A., Shaheen, A., Rajavashisth, T.B., AND Detrano, R.C..(2004). Genetic Determinants of Arterial Calcification Associated With Atherosclerosis.Mayo Clin Proc., 79 , 197-210 Frink, R.J..(2002).Calcification:a physiologic defense. In: Inflammatory Atherosclerosis. Ed. Available at: http://www.NCBI.com/bookshelf/Inflammatory Atherosclerosis/ Calcification:a physiologic defense .Accessed Oct 15,2002. Gerber,T.C..(2009). Diagnostic and prognostic implications of coronary artery calcification detected by computed tomography. alcif Tissue Int.,91, 123-137 Golledge, J., McCann, M., Mangan, S., Lam, A. and Karan, M.. (2004).Osteoprotegerin and osteopontin are expressed at high concentrations within symptomatic carotid atherosclerosis. Stroke., 35 , 1636-1641. Keelan, P.C., Bielak, L.F., Ashai, K., Jamjoum, L.S., Denktas, A.E., Rumberger, J.A., Peyser, P.A. and Schwartz, R.S..(2001). Long-term prognostic value of coronary calcification detected by Electron-Beam Computed Tomography in patients undergoing coronary angiography. Circulation ., 104 , 412-417 Ketteler, M. and Giachelli,C..(2006).Novel insights into vascular calcification. Kidn Inter.,70 , S5–S9. Kiechl, S., Schett, G., Schwaiger, J., Seppi, K., Eder, P., Egger, G., Santer, P., Mayr, A., Xu, Q. And Willeit, J..(2007). Soluble receptor activator of nuclear factor-kappa B ligand and risk for cardiovascular disease. Circulation.,116 , 385-391. Lim, M.C.L., Wong, T.W., Yaneza, L.O., De Larrazabal, C., Lau, J.K., and Boey, H.K..(2005). Non-invasive detection of significant coronary artery disease with multi-section computed tomography angiography in patients with suspected coronary artery disease. Arterioscler Thromb Vasc Biol.,31 , 937-952. Rackley,C.E., Weissman,N.J.. (2009).The role of plaque rupture in acute coronary syndromes. Arterioscler Thromb Vasc Biol.,54 , 743-759. Rackley, C.E..( 2009 ). Pathogenesis of atherosclerosis. Atherosclerosis .,202, e167- e174 Sandberg, W.J., Yndestad, A., Oie, E., Smith, C., Ueland, T., Ovchinnikova, O., Robertson, A.K., Muller, F., Semb, A.G., Scholz, H., Andreassen, A.K., Gullestad, L., Damas, J.K., Froland, S.S., Hansson, G.K., Halvorsen, B. and Aukrust, P.,( 2006) . Enhanced T-cell expression of RANK ligand in acute coronary syndrome: possible role in plaque destabilization. Arterioscler Thromb Vasc Biol.,26 , 857-863 Sattler, A.M., Schoppet, M., Schaefer, J.R. and Hofbauer, L.C..( 2004). Novel aspects on RANK ligand and osteoprotegerin in osteoporosis and vascular disease. Calcif Tissue Int.,74 , 103-106. Schoppet, M., Preissner, K.T and Hofbauer, L.C..(2002). RANK ligand and osteoprotegerin: paracrine regulators of bone metabolism and vascular function. Arterioscler Thromb Vasc Biol.,22 , 549-553. Schoppet, M., Sattler, A.M., Schaefer, J.R., Herzum, M., Maisch, B. and Hofbauer, L.C.. (2003). Increased osteoprotegerin serum levels in men with coronary artery disease. J Clin Endocrinol Metab.,88 , 1024-1028. Schoenhagen, P. and Nissen, S.E..(2005). Intravascular ultrasonography: Using imaging end points in coronary atherosclerosis trials. Cleve clin med ., 72 ,487-494 Ueland, T., Jemtland, R., Godang, K., Kjekshus, J., Hognestad, A., Omland, T., Squire, I.B., Gullestad, L., Bollerslev, J., Dickstein, K. and Aukrust, P.. (2004). Prognostic value of osteoprotegerin in heart failure after acute myocardial infarction. J Am Coll Cardiol .,44 , 1970-1976. Wilterdink,J.L., Furie ,K.L.,Kistler,J.P..(2009). Pathophysiology of symptoms from carotid atherosclerosis. Arterioscler Thromb Vasc Biol., 36 , 1394-1405 Table4:Correlation between OPG serum concentration with total coronary artery calcification Table5:Correlation between RANKL:OPG ratio, serum concentration of OPG and RANKL with LAD, RCA, LMCA and Cx coronary artey calcification Figure 1: Correlation between RANKL:OPG ratio with coronary artey calcification