Infections of the Labyrinth
390 likes | 671 Vues
2. Infections of the Labyrinth. Labyrinthitis: inflammation of the inner earMultiple etiologies: infectious, autoimmune, systemic disease, traumaInfectious agents include bacteria, viruses, fungus and protozoa.. 3. Labyrinthitis. Vestibular manifestations (vertigo)Cochlear manifestations (hea

Infections of the Labyrinth
E N D
Presentation Transcript
1. 1 Infections of the Labyrinth Sam J. Cunningham, MD, PhD
Arun Gadre, MD
UTMB Dept of Otolaryngology
February 2004
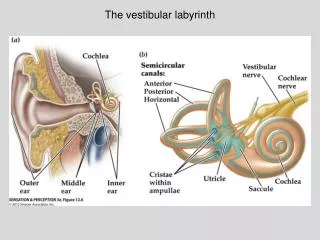
2. 2 Infections of the Labyrinth Labyrinthitis: inflammation of the inner ear
Multiple etiologies: infectious, autoimmune, systemic disease, trauma
Infectious agents include bacteria, viruses, fungus and protozoa.
3. 3 Labyrinthitis Vestibular manifestations (vertigo)
Cochlear manifestations (hearing loss)
Both
4. 4 Labrynthitis Infection usually occurs by one of three routes:
From the meninges
From the middle ear space
Hematogenous spread
5. 5 Labyrinthitis Meningogenic: through the IAC, cochlear aqueduct, both (bilateral)
Tympanogenic: extension of infection from the middle ear, mastoid cells or petrous apex-most common through the round or oval window (unilateral)
Hematogenous: least common
6. 6 Bacterial Infections Two types of labyrinthitis associated with bacterial infections:
Toxic Labyrinthitis
Suppurative Labyrinthitis
7. 7 Bacterial Infections Toxic Labyrinthitis: results from a sterile inflammation of the inner ear following an acute or chronic otitis media or early bacteria meningitis.
Toxins penetrate the round window, IAC, or cochlear aqueduct and cause an inflammatory reaction in the perilymph space.
8. 8 Bacterial Infection Toxic Labyrinthitis produces mild high frequency hearing loss or mild vestibular dysfunction
Treatment: Antibiotics for precipitating otitis, possible myringotomy.
9. 9 Bacterial Infection Suppurative Labyrinthitis: direct invasion of the inner ear by bacteria.
From otitis or meningitis
10. 10 Bacterial Infection Suppurative Labyrinthitis: 4 stages
Serous or irritative: production of Ig rich exudates in the perilymph
Acute or purulent: bacterial and leukocyte invasion of the perilymphatic scala-end organ necrosis
Fibrous or latent: proliferation of fibroblasts and granulation tissue in the perilymph
Osseous or sclerotic: new bone deposition throughout the involved labyrinth
11. 11 Bacterial Infection Purulent Labyrinthitis: medical emergency
Meningitis or Otitis symptoms
Hospitalization, hydration, vestibular suppressants and iv antibiotics
12. 12 Bacterial Meningitis H. influenza B, N. meningitidis, S. pneumoniae
Hib vaccine: 55% decrease in cases
Pneumococcus now predominant org.
13. 13 Bacterial Meningitis Postmeningitis hearing loss 10-20%
Bilateral, severe to profound, permanent
14. 14 Syphilis Treponema pallidum
Diagnosis by FTA-ABS and confirmed by Western Blot.
Congenital or Acquired
15. 15 Syphilis Acquired: SNHL during secondary or tertiary
Congenital:
Early: high fetal and infant mortality
Late SNHL+/- vestibular symptoms
16. 16 Viral Infections Congenital Infection
Systemic viral illness
Isolated involvement of inner ear
17. 17 Cytomegalovirus Most common congenital infection in US
Most common infectious cause of congenital deafness
Low birth weight, jaundice, hepatosplenomegaly, petechiae, microcephaly and psychomotor retardation.
65% w SNHL-bilateral, severe to profound
18. 18 CMV Diagnosis by isolating virus from urine during first few weeks of life.
Virus isolation form cord blood
No treatment: acyclovir may decrease amount of shedding, gancyclovir & foscarnet not approved during pregnancy.
19. 19 Rubella 1969 58/100000
1983 0.5/100000
Decline due to vaccine
Congenital rubella: cataracts, heart malformations and SNHL, others
Dx by viral culture
No treatment; prevention only
20. 20 Mumps Paramyxovirus
Parotitis, orchitis, meningoencephalitis, and in 0.05% of cases-hearing loss.
Hearing loss at end of first week of parotitis, unilateral and range from mild, high frequency SNHL to profound SNHL.
Vestibular involvement is uncommon
21. 21 Measles Rubeola virus
Systemic illness w rash, conjunctivitis, and mucosal Koplik spots.
Measles induced hearing loss is 1/1000 cases
Measles less common 2nd to vaccine
22. 22 Measles Encephalitis in 0.1% of cases w overall mortality rate of 15%, with 25% of survivors with SNHL.
SNHL seen in conjunction with rash.
Sudden onset
Varies from mild to profound HF SNHL
Unilateral or bilateral
PERMANENT
70% have vestibular losses also
23. 23 Varicella-zoster Primary vzv=chicken pox
HL w chicken pox = CHL 2nd to MEE
Reactivation=zoster
Herpes zoster oticus= Ramsay Hunt syndrome, reactivation from the geniculate ganglion of CN VII. Painful vesicles.
1/3 have auditory or vestibular symptoms-HFHL, hyperacusis, tinnitus, vertigo
24. 24 Herpes simplex Labyrinthine infection by:
Reactivation in the spiral ganglion=SSNHL
Extension of the meningoencephalitis along CN VIII to the labyrinth=acquired SNHL
25. 25 HSV HSV-1 &2 can infect labyrinth. Animal models of ISSNHL. ??Humans.
Neuroepithelial cells of the cochlea, utricle, saccule, and semicircular canals infected with HSV
Circumstantial evidence only
26. 26 Human Immunodeficiency virus Auditory and vestibular complaints rare in AIDS patients
Some w hearing loss, tinnitus and vertigo
Thought to be result of opportunistic infections (CMV, HSV), ototoxic drugs, neoplasm of inner ear.
27. 27 Fungal Infections Fungal labyrinthitis is exceedingly rare outside the context of host immunocompromise.
High risk: diabetics, chemo therapy, organ transplant recipients, AIDS patients
Agents include Mucor, Cryptococcus, Candida, Aspergillus, and Blastomyces
Hearing loss is severe and permanent
28. 28 Protozoa Toxoplama gondii most common
Acquired infection usually asymptomatic
Congenital infection may lead to severe malformations of fetus
Triad of chorioretinitis, hydrocephalus, intracranial calcifications
May also have microcephaly, cataracts, micropthalmia, jaundice, and hsm.
3000 cases annually
29. 29 Toxoplasma 75% asymptomatic at birth
15% ocular problems
10% severe malformations
85% of symptomatic infants at birth will later develop decreasing visual acuity, decreased intellectual function, hearing loss or precocious puberty.
30. 30 Toxoplasma Screening test to determine fetal infection
PCR analysis of amniotic fluid
IgM assays
Quantitative maternal/fetal IgG analysis of cord blood
31. 31 Toxoplasma Treatment
Prenatal tx reduces both transmission and severity of illness in the fetus
Combination of pyrimethamine and sulfonamide
Neonates with documented infection should be given tx for 1st year of life + folic acid supplements
32. 32 Clinical Presentation Pts present with only auditory dysfunction-acute cochlear labyrinthitis
Pts present with only vestibular dysfunction-acute vestibular labyrinthitis
Both-acute cochleovestibular labyrinthitis
33. 33 Clinical presentation Acute cochlear labyrinthitis, aka idiopathic sudden sensory neural hearing loss (ISSNHL)
Defined as minimum of 30dB deficit in three contiguous frequencies over a period of less than 3 days in a previously healthy person.
3 pathologic theories: viral infection, vascular phenomenon, intralabyrinthine membrane rupture.
Much circumstantial evidence of viral etiology
34. 34 Acute cochlear labyrinthitis Treatment is steroids. Studies have shown no benefit of steroids and antivirals.
30-70% have complete recovery of hearing.
Prognosis related to age, time from onset to presentation, type of audiogram, presence of vestibular symptoms
<40 years
Seen within 10 days
Started on steroids within 10 days
35. 35 Clinical presentation Acute vestibular labyrinthitis, aka vestibular neuritis
Defined as sudden unilateral vestibular weakness in the absence of concomitant auditory or CNS dysfunction in a previously healthy person
36. 36 Acute vestibular labyrinthitis Diagnostic criteria:
An acute, unilateral, peripheral vestibular disorder w/o associated hearing loss
Occurrence predominantly in middle age
A single episode of severe, prolonged vertigo
Decreased caloric response in the involved ear.
Complete subsidence of the symptoms within 6 months
37. 37 Acute vestibular labyrinthitis Treatment is supportive and includes hydration, antiemetics, and vestibular suppressants.
38. 38 References
Gulya, AJ Infections of the Labyrinth. Head and Neck Surgery-Otolarygology, BJ Bailey ed. Philadelphia. 2001.
Rosen, EJ Infections of the Labyrinth. UTMB Dept of Otolaryngology Web site in �Dr. Quinns Online Textbook and Grand Round Archives. 2000.
Stokroos, RJ Antiviral treatment of idiopathic sudden sensorineural hearing loss: a prospective, randomized, double-blinded clinical trial. Acta Oto-Laryngologica. 118(4):488-95, Jul 1998.
Stokroos, RJ The etiology of idiopathic sudden sensorineural hearing loss. Experimental herpes simplex virus infection of the inner ear. Am J of Otology. 19(4): 447-52, Jul 1998.
Paparella, MM. Labyrinthitis. Pp 81-92. June 12, 1978.
Satoh, H. Proinflammatory cytokine expression in the endolymphatic sac during ear inflammation. Jaro. 4(2): 139-47, Jun 2003.
Westerlaken, BO. Treatment of idiopathic sudden sensorineural hearing loss with antiviral therapy: a prospective, randomized, double blind clinical trial. Ann Oto, Rhino, Laryn. 112(11):993-1000. Nove 2003.
Arbusow V. HSV-1 not only in human vestibular ganglia but also in the vestibular labyrinth. Audiology and Neuro-Otology. 6(%):259-62, Sept. 2001.
Furman, J. Vestibular Disorders. 2nd ed. New York. Oxford Pub. 2003.