Download
1 / 27
270 likes | 435 Vues
Kathryn Anastos, M.D. Natural History of HIV Infection and Response to Antiretroviral Treatment in Women. The Body PRO Coverage of the 15th Conference on Retroviruses and Opportunistic Infections (CROI 2008) February 3-6, 2008 Boston, Mass. Faculty: Kathryn Anastos, M.D.

E N D
Kathryn Anastos, M.D. Natural History of HIV Infection and Response to Antiretroviral Treatment in Women The Body PRO Coverage of the 15th Conference on Retroviruses and Opportunistic Infections (CROI 2008) February 3-6, 2008 Boston, Mass. Faculty: Kathryn Anastos, M.D. Cal Cohen, M.D., M.S. David Wohl, M.D. Natural History of HIV Infection and Response to Antiretroviral Treatment in Women: A Summary of Key CROI 2008 Research
Faculty Kathryn Anastos, M.D. Kathryn Anastos, M.D., is the Executive Co-Director for Clinical and Scientific Programs of WE-ACTx (Women's Equity in Access to Care and Treatment, a community-based organization committed to providing HIV primary care, including antiretroviral therapy, to female survivors of genocidal rape in Rwanda. She has also developed and serves as the Principal Investigator of the Rwandan Women's Cohort Study (RWISA), funded by the U.S. National Institutes of Health (NIH). She is currently Professor of Medicine, Epidemiology and Population Health at Albert Einstein College of Medicine, Bronx, N.Y. Additionally, since 1993, Dr. Anastos has served as the Principal Investigator for the New York City/Bronx Consortium of the Women's Interagency HIV Study (WIHS), also funded by NIH. Cal Cohen, M.D., M.S. Dr. Cal Cohen is the research director of Harvard Vanguard Medical Associates and Community Research Initiative of New England in Boston, Mass. He is also a clinical instructor at Harvard Medical School. In addition, he works as an HIV clinical management consultant and internist at Harvard Pilgrim Health Care. Dr. Cohen holds appointments at Brigham and Women's Hospital and Beth Israel Hospital, both in Boston, Mass. In addition to caring for HIV-infected patients and directing clinical research at a large HIV community-based research site, Dr. Cohen is actively involved in evaluating new antiretroviral therapies, the durability and longevity of the benefits from such therapies and issues regarding compliance and adherence. Dr. Cohen has served as a consultant to or has received honoraria or research support from Abbott Laboratories, Boehringer-Ingelheim, Bristol-Myers Squibb, Gilead Sciences, GlaxoSmithKline and Tibotec. David Wohl, M.D. Dr. Wohl is an associate professor of medicine at the University of North Carolina at Chapel Hill, and co-directs HIV services for the North Carolina Department of Corrections. Dr. Wohl is an investigator in the NIAID-sponsored AIDS Clinical Trials Group (ACTG) and a member of the ACTG Complications of HIV Disease Research Agenda Committee. His research focuses on metabolic and infectious complications of HIV and its therapies, as well as issues related to medication adherence and access to care—particularly among incarcerated inmates with HIV infection. Dr. Wohl has served as a consultant to or has received honoraria or research support from Abbott Laboratories, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead, Merck & Co, Roche Laboratories and Tibotec. This activity is supported by an educational grant from
About This Slide Presentation • This presentation was created to accompany The Body PRO's summary of key research presented at CROI 2008, featuring reports by Kathryn Anastos, M.D., Cal Cohen, M.D., M.S., and David Wohl, M.D. For more information about this program, please visit us on the Web at: TheBodyPRO.com/CROI2008 • Please feel free to use this slide presentation for personal reference or for your own presentations; however, we ask that you not modify any aspects of the slides contained within this presentation, so proper attribution can be retained. If you would like to publish all or part of this presentation, or repost any of these slides online, permission must first be obtained from Body Health Resources Corporation. • Our gratitude goes out to all the researchers who granted permission for their slides to be adapted for this presentation.
Natural History of HIV Infection and Response to Antiretroviral Treatment in Women
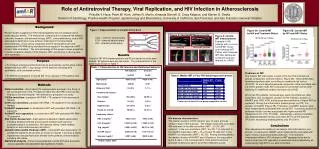
Regression Model Adjusted for Race, Country and History of AIDS Male-Female Mean Viral Load Difference (Log10 Copies/mL) Exact Screening CD4+ Lymphocytes (mm3) Adapted from Beatriz Grinsztejn et al. CROI 2008; abstract 672.
Cox Proportional Hazards Model of Factors at Enrollment Associated With Death Among HIV-Infected Persons Attending the CCC in Nashville, Tenn.a aIn addition to the variables listed, the following variables were included in the multivariate model: ART/HAART exposure prior to first visit, baseline CD4+ percent, baseline HIV-1 RNA level. These variables were not significantly associated with death. Diana Lemly et al. CROI 2008; abstract 810. Reprinted with permission.
Cox Proportional Hazards Model of Factors, Including HAART Utilization, Associated With Deatha aIn addition to the variables listed, the following variables were included in the multivariate model: ART/HAART exposure prior to first visit, baseline CD4+ percent, baseline HIV-1 RNA level and ART exposure prior to initiation of HAART. These variables were not significantly associated with death.bUnivariate HR 0.45 (P < 0.001) Diana Lemly et al. CROI 2008; abstract 810. Reprinted with permission.
Comparison of Factors 12 Months After HAART Between African and European Americans Amy Weintrob et al. CROI 2008; abstract 809. Reprinted with permission.
Univariate and Multivariate Predictors of CD4+ Change From Pre-ART to Longest Follow-Up (n = 400) Kathryn Anastos et al. CROI 2008; abstract 667. Reprinted with permission.
Univariate and Multivariate Predictors of Change in HIV-1 RNA From Pre-ART to Longest Follow-Up (n = 229) Kathryn Anastos et al. CROI 2008; abstract 667. Reprinted with permission.
Distribution of the Underlying Causes of Death in HIV-Infected Adults, According to Their Gender Men Women 2000n = 964 2005n = 1042 Adapted from Mojgan Hessamfar-Bonarek et al. CROI 2008; abstract 666.
Longer Cumulative Exposure to NRTIs Was Associated With Greater IR in HIV-Infected Women *1,614 HIV-infected women contributed a total of 7,981 person-visits of follow-up including the index visit†Anti-log of coefficient of exposure group from regression model ‡Adjusted for cumulative number of NRTI, PI, or NNRTI reported from WIHS baseline through the visit prior to index, WIHS cohort status (1994-1995 or 2001-2002), race, baseline HCV antibody status, family history of diabetes, and age, smoking status, BMI, CD4 count, menopause assessed at visit immediately prior to index; if data for a particular variable was missing at visit immediately prior to index then data concurrent with index visit was used; 1,482 women contributing 7,529 person-visits were included in analysis Phyllis Tien et al. CROI 2008; abstract 933. Reprinted with permission.
Sex Differences Between Regimens for Time to Virologic Failure and Time to Treatment Limiting Toxicity Adapted from Sharon Riddler et al. CROI 2008; abstract 776.
Multivariate* Association of Immune Markers With HIV-1 Genital Shedding *Adjusted for ARV therapy, genital infection and CD4+ or HIV viral load. LaShonda Spencer et al. CROI 2008: abstract 674. Reprinted with permission.
Effect of Vaginal Flora on CVL HIV RNA:Cross-Sectional Analysis – Adjusted for Log10 Plasma HIV RNA Jane Hitti et al. CROI 2008; abstract 27LB. Reprinted with permission.
H2O2+ Lactobacillus Acquisition/Loss:Effect on Log10 CVL HIV RNA Jane Hitti et al. CROI 2008; abstract 27LB. Reprinted with permission.
Male Circumcision and HSV-2 Acquisition Over a 24 Month Follow-Up RR 0.76P = 0.019CI 0.50 to 0.96 RR 0.72P = 0.07CI 0.50 to 1.03 RR 0.53P = 0.001CI 0.35 to 0.78 RR 0.63P = 0.015CI 0.44 to 0.91 In almost all sociodemographic and behavioral subgroups, the relative risk of HSV-2 incidence was lower in the circumcision arm. Adapted from Aaron Tobian et al. CROI 2008; abstract 28LB.
Vaginal Infections at 12 Month Follow-Up By Husband’s Study Arm PRR 0.53CI 0.33 to 0.85 PRR 0.31CI 0.18 to 0.54 PRR 0.80CI 0.71 to 0.89 There was a significant reduction of progression from normal flora to BV and reduced persistence of BV from enrollment to follow-up in wives of circumcised men. Adapted from Aaron Tobian et al. CROI 2008; abstract 28LB.
Male-to-Female HIV Transmission by Study Arm for Wives Concurrently Enrolled With Their Partner: Intent-to-Treat Analysis Includes one crossover in control arm and eight crossover men in MC arm. Adapted from Maria J. Wawer et al. CROI 2008; abstract 33LB.
Male-to-Female Transmission by Timing of Wound Healing and Resumption of Sex, 0 to 6 Month Follow-Up Interval Excludes uncircumcised men (8) and couples who did not resume sex (3) Adapted from Maria J. Wawer et al. CROI 2008; abstract 33LB.
HIV Acquisition Events and Rate Per 100 Person-Years by Gender Overall Hazard Ratio: 1.16 (95% CI 0.83 to 1.62) aExcluding time off study drug use due to pregnancy. HIV incidence for acyclovir was 3.8/100 person-years and for placebo 3.3/100 person-years. Overall Hazard Ratio: 1.13 (95% CI 0.81 to 1.59). Adapted from Connie Celum et al. CROI 2008; abstract 32.
Pharmacokinetic Results Julie Dumond et al. CROI 2008; abstract 135LB. Reprinted with permission.
DMPA and HIV Acquisition Elizabeth Stringer. CROI 2008; abstract 94. Reprinted with permission.
OCPs and HIV Acquisition Elizabeth Stringer. CROI 2008; abstract 94. Reprinted with permission.
Other Studies of HIV Disease Progression and HC Elizabeth Stringer. CROI 2008; abstract 94. Reprinted with permission.
Epithelial Disruption Intact genital tract mucosal epithelium is impervious to HIV Disrupted epithelium allows HIV to migrate across the barrier and infect target cells HIV-1 Mucosal epithelium Disruptive microbicide (N-9) T-cells Betsy Herold et al. CROI 2008: abstract 26. Reprinted with permission.