Download
1 / 43
430 likes | 627 Vues
AGEING POPULATION AND THE FUTURE OF HEALTH CARE PLANS An international perspective. J. François Outreville UNCTAD Visiting Professor SUFE Adjunct Professor HEC Montréal. AGEING POPULATION AND THE FUTURE OF HEALTH CARE PLANS. Background information on health care systems

E N D
AGEING POPULATION AND THE FUTURE OF HEALTH CARE PLANSAn international perspective J. François Outreville UNCTAD Visiting Professor SUFE Adjunct Professor HEC Montréal
AGEING POPULATION AND THE FUTURE OF HEALTH CARE PLANS • Background information on health care systems • The increasing role of private health plans • Challenges to come • Ageing revisited
Health care expenditure as % of GDPSource: OCDE Health Data 2005A comparison between 1980 and 2003
The Growth of HCE today:examples • Rapid Growth USA, Greece, Portugal, Korea, Turkey • Stabilized Netherlands, UK, Austria Germany, Canada • No growth Sweden, Finland, Denmark
Health care expenditure:the size of public sectorsSource: OCDE Health Data 2006
Out of Pocket expenditure and Private Health insurance: No relationshipSource: OCDE Health Data 2004
Bismarck’s principle Beveridge’s principle State budget Private insurers under state control Health Insurance systems: principles
Increasing role of Private Insurance HCE as % GDPSource: OCDE Health Data 2004
Population covered by Private InsuranceSource: OCDE Health Data 2004
Primary coverage Risks not covered by the public scheme (supplementary insurance) Complementary insurance Access to private market (substitutable) Classification of Private Health Insurance Plans
The challenges • Health insurance schemes are being dragged into increasing expenditure by demographic changes and improvements in medical treatment. • A growing interest in the problem of the long-term survival of public schemes is paralleled by a desire to arrive at an acceptable compromise between equity and efficiency, between meeting individual needs and controlling collective expenditure. • The European social philosophy of each contributing according to his means is radically opposed to the individualistic North American arrangement whereby everyone takes out insurance according to his needs.
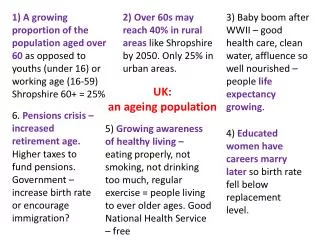
The problems • Budget deficits • Tax limits • Cost of new medical treatments • Ageing of the population • Decreasing labor force
Several options are available • « Opt out » (Germany) • Voluntary or compulsory • Public scheme covers only catastrophic risks • Case of LTC (Netherlands and Germany) • Higher and competitive premiums but subsidies for lower income • Case in Switzerland • Covers only basic health treatments (Doctors & Hospitals) • Some treatments excluded (drugs in Canada) • Open markets to free choice and free trade • Cultural barriers • Portability of insurance coverage
Satisfaction rate for public schemes is highSource: OCDE Health Data 2004
AGEING POPULATION AND THE FUTURE OF HEALTH CARE PLANS • “The first and primary cause of this crisis is once again the ageing of the population…” (Longman, 1987)
Ageing of the population When Bismarck devised the social security contract for Germany, the official pension age was 65 and life expectancy 45. Keeping the same ratio, retirement age today should be at 98. Old age estimated to be at 75 years in 1985, will be 82 years by 2040: an annual gain of 1.5 months
Ageing of population and health care expenditure Source : S. Jacobzone (2003)
Ageing and HCE: What is the relationship? Hypotheses: • The probability of initiating a treatment episode is independent of age. • Medical expenditure per treatment episode increases with age. • Medical expenditure increases sharply with closeness to death regardless of age. • Medical expenditure before death increases/decreases with age?
Lubitz and Riley, New England J. of Medicine, 1993 Zweifel, Felder and Meier, Health Economics, 1999 Felder and Schmitt, J. Health Economics, 2000 Hogan, Lunney, Gabel and Lynn, Health Affairs, 2001 Levinsky et al., J. of American Medical Association, 2001 Outreville, Geneva Papers on Risk and Insurance, 2001 Seshamani and Gray, Applied Health Economics and Health Policy, 2003 Seshamani and Gray, J. of Health Economics, 2004 Outreville, Applied Health Economics and Health Policy, 2005 References:
Empirical evidence • UN health insurance plan • 15,000 insured persons • 2 periods 1996-1997 and 2000-2002
Hospital HCE in the 12 months preceding deathBy class of age in CHF
Ageing and HCE: What is increasing with age? • Trends in medical expenditure are influenced by trends in disability and product innovation. • Product innovation focus on increasing quality of life at higher ages. • LTC expenditure before death increases with age
Cost of pharmaceuticals by age • On average from 13% to 16% of total HCE within 10 years
Nursing and Long-Term Care (LTC) • Average number of days in an hospital has been reduced from 10 to 7 days within 10 years
AGEING AND THE FUTURE OF HEALTH CARE PLANS • SUSTAINABILITY • Individuals are living longer in good health. • People over 95 are on average in better state of health than those over 85 (absence of chronic diseases).
Mortality and disability scenariosT= Total expected lifeH= Healthy expected life Source: E. Pitacco (2002)
Negative factors • Medical expenditure per treatment episode increases with age. • Trends in medical expenditure are influenced by trends in disability and product innovation. • Product innovation focus on increasing quality of life at higher ages. • The traditional family structure continue to change
Declines in disability rates (-1% per year) even at older age (85+). Instrumental activities of daily living (IADLs) are easier to perform today than 20 years ago. Product innovation may change the trends Improving trends
AGEING AND THE FUTURE OF HEALTH CARE PLANS • SUSTAINABILITY • Individuals are living longer in good health • EQUITY • Health Care or Good Health • Health Care or Long Term Care • Health Care or Terminal Care • INNOVATION • Health Insurance or Life Insurance (terminal illness) • Traditional Insurance or Alternative Risk Transfer
AGEING POPULATION AND THE FUTURE OF HEALTH CARE PLANS • “As people are living longer, the hope is that they will also live healthily.”