Download
1 / 54
540 likes | 727 Vues
The Value of Observational Research A Case Study Approach. Hal V. Barron, MD. Review what we can learn from observational data Examine associations and attempt to speculate on causality when RCTs are not feasible when RCTs are unethical (Does smoking really cause cancer?)

E N D
The Value of Observational Research A Case Study Approach Hal V. Barron, MD
Review what we can learn from observational data Examine associations and attempt to speculate on causality when RCTs are not feasible when RCTs are unethical (Does smoking really cause cancer?) when the sample size needed for a RCT is prohibitive Examine associations for hypothesis generation Describe what is happening in the “real world” Safety surveillance : Identification of rare events or subgroup analysis Drug utilization patterns Natural history of disease Efficacy vs Effectiveness Overview
Studies have demonstrated the importance of establishing and maintaining a patent infarct related artery in the setting of acute myocardial infarction (AMI) complicated by cardiogenic shock. The purpose of the present study was to determine whether the use of Intra-aortic baloon pumping (IABP) is associated with a survival advantage in patients with AMI complicated by cardiogenic shock. Why not do a RCT??? Examine associations and attempt to speculate on causality when RCTs are not feasible
Using data from the National Registry of Myocardial Infarction 2 (NRMI 2), we evaluated 23,180 patients who presented with or developed cardiogenic shock during the hospitalization. National Registry of Myocardial Infarction (NRMI) : IABP Use and Outcome
Review what we can learn from observational data Examine associations and attempt to speculate on causality when RCTs are not feasible when RCTs are unethical (Does smoking really cause cancer?) when the sample size needed for a RCT is prohibitive Examine associations for hypothesis generation Describe what is happening in the “real world” Safety surveillance : Identification of rare events or subgroup analysis Drug utilization patterns Natural history of disease Efficacy vs Effectiveness Overview
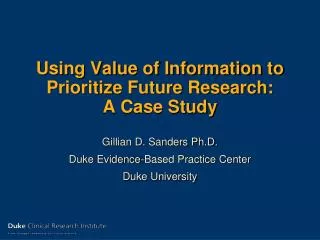
Do beta-blockers reduce intra-cranial hemorrhage ICH rates when given immediately following tPA for AMI Does this meet the FINER criteria? What is the rate of ICH following tPA? Is a 30% reduction meaningful? What size trial would need to be conducted? Examine associations and attempt to speculate on causality when RCTs are not feasible
NRMI: BB Use and ICH Unadjusted ICH Rate (%) AGE
NRMI: BB Use and ICH Unadjusted ICH Rate
Multivariate Analysis: Effect of Drug Therapy Administered Within 24 Hours on Intracranial Hemorrhage Rate Medication Adjusted OR (95% Cl) blocker 0.69 (0.57-0.84)* ACE inhibitor 0.75 (0.55-1.03) Calcium channel antagonist 1.27 (0.98-1.64) Lidocaine 0.93 (0.76-1.13) Intravenous magnesium 1.05 (0.76-1.45) Intravenous nitroglycerin 0.86 (0.69-1.09) *p<0.001. Cl = confidence intervals; OR = odds ratio; other abbreviation as in Table 1. NRMI and Beta-blocker Use
Review what we can learn from observational data Examine associations and attempt to speculate on causality when RCTs are not feasible unethical studies sample size is prohibitive Examine associations for hypothesis generation Describe what is happening in the “real world” Safety surveillance : Identification of rare events or subgroup analysis Drug utilization patterns Natural history of disease Efficacy vs Effectiveness Overview
Immunological Mechanisms Involved in Allergic Disease Sensitization Re-Exposure Allergen Allergen Environment Submucosa Antigen- Presenting Cell Productionof Antigen- Specific IgE MHC Class II Protein and Epitope ClinicalEffects Mast Cell Degranulation Asthma, Rhinitis, Urticaria + Th2-Cell B-Cell Mediators
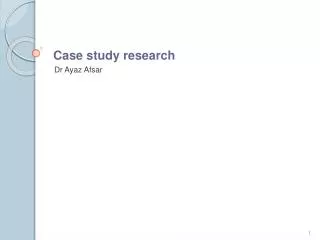
IgE and Asthma Relationship in Adults 40 N = 2657 20 Asthma 10 Odds ratio 5 2.5 Rhinitis 1 0.32 1 3.2 10 32 100 320 1000 3200 Serum IgE (IU/mL) Burrows B, et al. N Engl J Med. 1989;320:271–277.
Omalizumab Placebo Patients With 1 Significant Asthma Exacerbations 37% 58% 30% 40 P = .009 P < .001 P = .095 30.5 30 23.3 23.0 Patients, % 20 16.0 14.6 12.8 10 n =268 257 274 272 225 109 0 US (008) International (009) Pediatric (010) Distribution of AEEs per patient P = .006 P < .001 P = .093 Significant asthma exacerbation = episode requiring course of oral CS or doubling dose of ICS
Background: Patients with elevated white blood cell (WBC) counts during acute myocardial infarction (AMI) have a higher risk of adverse outcomes. Objectives: The goal of this study was to determine the relationship between the WBC count and angiographic characteristics to gain insight into this pathophysiology of this clinical observation. Methods: Angiographic and clinical data from 936 patients in the TIMI 10A and TIMI 10B trials was used to evaluate these relationships The Association Between White Blood Cell Count, Epicardial Blood Flow, Myocardial Perfusion, and Clinical Outcomes in the Setting of Acute Myocardial InfarctionHal V. Barron, M.D.; Christopher P. Cannon, M.D.; Sabina A. Murphy, M.P.H.; Susan J. Marble, M.S., R.N.; Eugene Braunwald, M.D.; and C. Michael Gibson, M.S., M.D.; for the TIMI 10 Study Group
Preventing “Diseases” of The Endothelium: The Role Of The Integrins
Results : The development of new congestive heart failure was associated with significantly higher WBC counts (13.3 8.9, n=64 vs 10.8 3.5, p<0.0001), an observation which remained significant in a multivariable model adjusting for all potential confounding variables (O.R. 1.2 per 1 unit increase in WBC count, p<0.001).
Review what we can learn from observational data Examine associations and attempt to speculate on causality when RCTs are not feasible unethical studies sample size is prohibitive Examine associations for hypothesis generation Describe what is happening in the “real world” Safety surveillance : Identification of rare events or subgroup analysis Drug utilization patterns Natural history of disease Efficacy vs Effectiveness Overview
ICH Risk following t-PA:NRMI 2 Gurwitz et al. 1998 Annals Int Med. 129; 597-604.
Initial reperfusion therapy (IRT) is beneficial for patients with acute myocardial infarction (AMI) A minority of patients with AMI receive IRT Underutilization could be related to: the absence of clear indications perceived contraindications physicians’ reluctance to prescribe IRT Background
To determine what percent of patients identified as having clear indications for initial reperfusion therapy (IRT) do not receive this life-saving therapy To identify patient subgroups who are at greatest risk for not receiving IRT Hypothesis
Methods - Study Population SymptomsHosp <6 hrs ST Segment or LBBB Contraindications to thrombolytic Rx No IRT N=20,319 IRT N=64,344
Reperfusion Therapy LBBB No CP Age > 75 Prior CHF Prior MI Prior Stroke Killip 3# Killip 2# Prior Angina Diabetes Female Prior Revasc. Anterior MI* Prior HTN Caucasian Current Smoker Prehospital ECG Sx < 3 hrs. Less Likely More Likely 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8
At least 31% of patients presenting with AMI are appropriate for IRT 1 in 4 patients appropriate for IRT do not receive this life-saving therapy The underutilization is particularly evident in the elderly, women and other patients at increased risk for in-hospital mortality Conclusions
Review what we can learn from observational data Examine associations and attempt to speculate on causality when RCTs are not feasible when RCTs are unethical (Does smoking really cause cancer?) when the sample size needed for a RCT is prohibitive Examine associations for hypothesis generation Describe what is happening in the “real world” Safety surveillance : Identification of rare events or subgroup analysis Drug utilization patterns Natural history of disease Efficacy vs Effectiveness Overview
Literature is conflicting about whether short-term mortality after MI is higher in women than in men after adjusting for age and other prognostic factors • Traditional approach: compare all the men and all the women, adjusting for age and other factors
Data Source Second National Registry of Myocardial Infarction (NRMI-2) 1,658 participating U.S. hospitals N=691,995 MI patients enrolled up to 1/31/98 Methods of Analysis :Multiple logistic regression with hospital death as outcome Traditional analysis approach: main effect of female sex after adjusting for age Test for sex-age interaction Sequential adjustment for other covariables • Specific Aims • To test the following hypotheses: 1. the mortality of women relative to men is not constant across ages 2. the younger the age of the patients, the higher the risk of death in women relative to men • To identify factors that may account for the higher mortality rates of women compared with men
WomenMen Mean age 72 66 History of MI (%) 24 28 History of CHF (%) 21 13 History of HTN (%) 59 47 History of diabetes (%) 33 25 Chest pain (%) 63 72 ST elevation (%) 38 42 CHF or cardiog. shock (%) 27 19 Hospital mortality (%) 17 11 RESULTSSelected Patient Characteristics by Sex
OR of Mortality Women Vs. Men (95% CI) Unadjusted 1.54 (1.51-1.57) Age adjusted 1.14 (1.12-1.17) Overall Effect of Female Sex on Mortality (traditional approach)
Demographic factors Non-White race Medicaid insurance Medical history Hx of CHF Hx of diabetes Hx of stroke Admission data Delay to presentation >6 hrs No ST elevation CHF, pulmonary edema Hypotension or cardiogenic shock Treatments No coronary reperfusion therapy No use of IV beta-blockers Factors Disproportionately more Common in Women at Younger Ages
Hospital Mortality Rates by Sex and Age (Unadjusted) Sex-Age Interaction: P<0.001
Effect of Female Sex on Mortality by Age (Unadjusted) 30 35 40 45 50 55 60 65 70 75 80 85 90 Age
Impact of Overall Adjustment Unadjusted OR (Women Vs. Men) Adjusted 30 35 40 45 50 55 60 65 70 75 80 85 90 Age
Summary / Conclusions • A higher risk of death in women relative to men is seen in the younger age groups only • There is a linear increase of risk for women relative to men going from older to younger age • The younger the patients’ age, the higher the risk of death of women relative to men • Adjustment for covariables explains only 1/3 of the higher mortality risk for women at younger ages
Review what we can learn from observational data Examine associations and attempt to speculate on causality when RCTs are not feasible when RCTs are unethical (Does smoking really cause cancer?) when the sample size needed for a RCT is prohibitive Examine associations for hypothesis generation Examine associations to identify treatment modifiers Describe what is happening in the “real world” Safety surveillance: Identification of rare events or subgroup analysis Drug utilization patterns Natural history of disease Efficacy vs Effectiveness Overview
Trials Comparing Primary PTCA With Fibrinolytic Therapy: PAMI Cohort 12.0 P=0.06 P=0.02 Grines CL, et al. N Engl J Med. 1993;328:673-679.
Trials Comparing Primary PTCA With Fibrinolytic Therapy: GUSTO-IIb Cohort Composite Outcome (%) P=0.033 P=NS GUSTO-IIb Angioplasty Substudy Investigators. N Engl J Med. 1997;336:1621-1628
Meta-analysis of Mortality Benefit With Primary PTCA Versus Fibrinolytic Therapy Rate % Study Group Absolute Risk Reduction, % (95% CI) Lytic Therapy Odds Ratio (95% CI) PTCA Streptokinase 4.0 5.9 0.66 (0.29 to1.50) 1.9 (-2.7 to 4.1) 3- to 4-hour t-PA 3.5 5.7 0.60 (0.24 to1.41) 2.2 (-2.2 to 4.3) Accelerated t-PA 5.0 7.2 0.68 (0.42 to 1.08) 2.2 (-0.5 to 4.0) Total 4.4 6.5 0.66 (0.46 to 0.94) 2.1 (0.4 to 3.4) Weaver WD, et al. JAMA. 1997;678:2093-2098.
Trials Comparing Primary PTCA With Fibrinolytic Therapy: MITI Cohort P=NS 0 0.5 1 1.5 2 2.5 3 3.5 4 Time After Discharge (years) Every NR, et al. N Engl J Med.1996;335:1253-1260.
4,939 nontransfer pts underwent PPTCA within 12 hrs from Sx onset 24,705 pts received tPA Lytic ineligable and shock pts were excluded PPTCA versus tPA :NRMI 2
Randomized Trial Results Versus Community-Setting Results: NRMI-2 Cohort n=2958, lytic eligible, no shock at presentation Percent P=NS P=NS Tiefenbrunn AJ, et al. J Am Coll Cardiol. 1998;31:1240-1245.
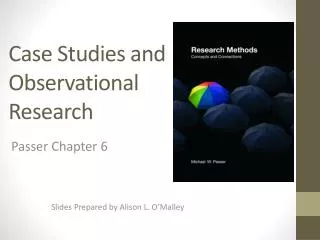
Mortality (%) Odds Ratio and 95% CI rt-PA PTCA Overall 5.4 5.2 STE or LBBB 1st ECG 5.3 5.5 Age < 75 yr. 3.4 3.5 Age > 75 yr. 16.5 14.4 Male 4.5 5.2 Female 9.6 8.9 Inferior MI 3.9 3.9 Anterior MI 7.6 7.1 Low Risk 2.9 2.8 Not Low Risk 7.5 7.4 0.5 1.0 1.5 rt-PA better PTCA better
Why might they differ? Efficacy vs Effectiveness