Download
1 / 54
540 likes | 669 Vues
Radiological examination of the urinary tract and retro-peritoneal space. DEPARTMENT OF ONCOLOGY AND RADIOLOGY PREPARED BY I.M.LESKIV. RENAL STRUCTURE AND FUNCTION.

E N D
Radiological examination of the urinary tract and retro-peritoneal space. DEPARTMENT OF ONCOLOGY AND RADIOLOGY PREPARED BY I.M.LESKIV
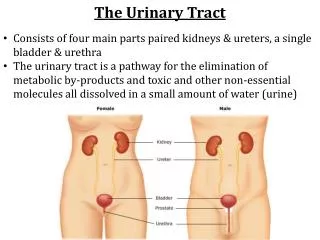
RENAL STRUCTURE AND FUNCTION • The kidneys control the volume, composition, and pressure of body fluids by regulating the excretion of water and solutes. They also influence red cell production and blood pressure by hormonal mechanisms. Urine is formed in the kidneys as an aqueous solution containing metabolic waste products, foreign substances, and water-soluble constituents of the body in quantities depending upon homeostatic needs.
Anatomy • The kidneys are bilateral, retroperitoneal structures, each consisting of an outer cortex and an inner medulla. The medulla is arranged into several cone-shaped or; pyramidal projections separated from each other by sections of cortex called renal columns. The bases of the pyramids face the cortex of the kidney while the apices (papillae) point toward the hilus and project into the renal pelvis. The; cortex contains glomeruli and tubules; the medulla, tubules only. • The kidneys possess numerous blood vessels and because of their low vascular resistance receive approximately 1200 ml of blood or 25% of the cardiac output each minute. • The major resistance to blood flow occurs in the glomerular capillary bed and is produced by a relatively high resistance in the efferent arterioles. However, changes in renal arterial pressure produce proportional variations in the afferent arteriolar resistance, which tends to preserve a constant renal blood flow (RBF) and glomerular capillary pressure; i.e., autoregulation. In addition to autoregulatioaj the renal circulation is controlled by extrinsic factors such as neurogenic (sympathetic) and hormonal (epinephrine, norepinephrine, and angiotensin) regulators. I
Sagittal section of the kidney. The upper half depicts the overall gross anatomic arrangement The lower half demonstrates the arterial supply.
The Nephron • The basic functional unit of the kidney is the nephron, a long tubular structure made up of successive segments of diverse structure and transport functions. It includes (1) a renal corpuscle (Bowman's capsule and the glomerulus, a tuft of capillaries), (2) a proximal tubule (convoluted and straight portion), (3) a hairpin loop (Henle's loop), (4) a distal tubule (straight portion, macula densa, and convoluted portion), and (5) a collecting duct system. There are approximately one million nephrons in each human kidney; 85% are cortical nephrons with short loops of Henle, and 15% are juxtamedullary nephrons with glomeruli near the cortical medullary junction and with long, thin, looping segments
Glomerular Filtration The glomerulus acts as an ultrafilter, allowing passage of water, electrolytes, and small organic molecules such as glucose, but not blood cells and large protein molecules. The ultrafiltrate produced by the glomeruli of both kidneys amounts to about 70 ml/min/sq m or 150 L/day/sq m; this rate is termed the glomerular filtration rate (GFR). About 99% of the glomerular filtrate is resorbed during passage through the renal tubules, with most of the resorption taking place in the proximal tubules. • The Concept of "Clearance" and the Measurement of GFR • A principal function of the kidney is to remove or "clear" various solutes from the blood which are not essential to the body, and to conserve those that the body requires. A solute is never totally removed from the blood in any one passage through the kidneys; rather, a portion is removed during each sweep of the blood through the renal system. Clearance may be defined as the volume of plasma which is completely cleared of a solute in a unit of time and is usually expressed in ml/min.Stated another way, the renal clearance of a substance represents the volume of blood that would have to pass through the nephrons within a given time period to provide the amount of that substance in the urine. Substances which are rapidly eliminated have a high clearance; those eliminated slowly, a low clearance.
Radiological examination of the urinary tract • The four basic examinations of the urinary tract are intravenous urography (IVU), computed tomography (CT), ultrasound and radionuclide examinations. Magnetic resonance imaging (MRI), arteriography and studies requiring catheterization or direct puncture of the collecting systems are limited to highly selected patients. • The IVU provides both functional and anatomical information. CT, MRI and ultrasound are essentially used for anatomical information; the functional information they provide is limited. The converse is true of radionuclide examinations where functional information is paramount. • Ultrasound is the first-line investigation to demonstrate or exclude hydronephrosis, particularly in patients with renal failure, and to diagnose renal tumours, cysts and abscesses. • Computed tomography is preeminent for staging renal tumours, for diagnosing or excluding trauma to the urinary tract and for showing pathology in the retroperitoneum.
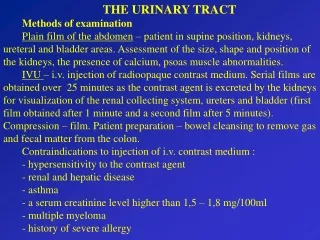
Radiographic Evaluation of the Urinary System • A plain x-ray of the abdomen (kidney, ureter, bladder [KUB]) is performed first to demonstrate the size and location of the kidneys. Since gastrointestinal and urinary system diseases tend to mimic each other, the x-ray may be helpful in differential diagnosis However, the renal outline can be obscured by bowel content, lack of perinephric fat, or a perinephric hematoma or abscess. This difficulty may be overcome by tomography. Congenital absence of a kidney may be suggested. If both kidneys are unusually large, polycystic kidney disease, multiple myeloma, lymphoma, amyloid disease, or hydronephrosis may be present If both are small, the end stage of glomerulonephritis or bilateral atrophic pyelonephritis must be considered. Unilateral enlargement should suggest renal tumor, cyst, or hydronephrosis, whereas a small kidney on one side is compatible with congenital hypoplasia, atrophic pyelonephritis, or an ischemic kidney Normally, the left kidney is 0.5 cm longer than its mate. • In 90% of cases, the right kidney is lower than the left because of displacement by the liver. The long axes of the kidneys are oblique to the spine and tend to parallel the borders of the psoas muscles. If both kidneys are parallel to the spine, the possibility of horseshoe kidneys should be considered. If only one kidney is displaced, a tumor or cyst should be consideredBecause an x-ray film is two-dimensional, a positive diagnosis of a stone in the urinary tract is practically impossible except in the instance of a staghorn calculus. However, suspicious opaque bodies may be noted in the region of the adrenal, kidney, ureter, bladder, or prostate. Oblique and lateral films, as well as visualization of the urinary tract with radiopaque fluids, are necessary in order to place the calcification specifically within these organs.
An excretory urogram is used to visualize the kidney and lower urinary tract. Studies are done by an IV infusion of a triiodinated benzoic acid derivative. The iodine molecule provides radiopacity, while the benzoic acid molecule is rapidly filtered by the kidney. After IV injection of a contrast agent, the drug becomes concentrated in the renal tubules within the first 5 min, providing a nephrogram. Later, the contrast agent appears in the collecting system, outlining the renal pelvis, the ureters, and finally the bladder. This ability to visualize the urinary system is dependent on adequate renal function and, to some degree, on the absence of an osmotic or water diuresis which would dilute the contrast agent. Therefore, the best radiograms are obtained in patients with a normal GFR who have been water-restricted. It is usually difficult to obtain an adequate study in patients with a BUN > 70 mg/dl or a plasma creatinine > 7 mg/dl. Excretory urograms are indicated when disease of the urinary tract is suspected. This test may be useful in investigating cysts and tumors of the kidneys (space-occupying lesions), infections of the kidney (distortion of the calyces), hydronephrosis, vesicoureteral reflux, hypertension, and Iithiasis. If renal injury is suspected, excretory urography should be done to make certain that the contralateral uninjured kidney is normal, and to obtain functional information about the injured kidney. Finally, excretory urograms are indispensable in infants, particularly males, for whom cystoscopy may be unduly traumatic.
The retrograde pyelogram is a procedure in which radiopaque agents similar to those used in excretory urography are introduced directly into the urinary tract following cystoscopy and catheterization of the ureter. The technic provides more intense opacification of the collecting and voiding system when the excretory urogram has been unsuccessful owing to poor renal function. Retrograde evaluation may also be indicated to assess the degree of ureteral obstruction or when the patient is allergic to IV radiopaque chemicals. • The cystogram is obtained as a part of the excretory urogram but may be unsatisfactory owing to poor opacification or incomplete filling. Controlled bladder filling utilizing a catheter (retrograde cystogram) is then necessary for adequate visualization. Retrograde cystograms are advisable for study of neurogenic bladder, bladder rupture, or recurrent urinary tract infections. Such causes as vesicoureteral reflux or vesical fistulas are best diagnosed by this technic. • The male urethra may be examined by the retrograde injection of a contrast agent, although the information needed is frequently seen in a voiding film after an excretory urogram. When the retrograde urethral injection is combined with this cystography, the combined procedure is called retrograde urethrocystography. • For special problems concerning the integrity of the renal blood supply, contrast media may be selectively injected into the arterial supply (arteriography) or the venous system (venography).
Renal Evaluation with Radioisotopes • Radionuclides which are selectively accumulated or secreted by the kidney permit evaluation of renal structure and function without introducing the hypertonic and chemical stress of IV contrast agents. Because of the trace amounts given, the danger of hypersensitivity is decreased and, with the use of rapidly decaying isotopes, the biologic damage from radiation is small The particular advantage of radioisotopic scintiphotography over x-rays is the ease with which radioisotope concentration can be estimated by counting radioactive disintegrations while a simultaneous image of radioisotope dilution is produced Thus, static as well as dynamic studies are possible While x-ray images are not readily susceptible to numerical quantitation, they do have a higher resolution than radioisotope images. All of the radiopharmaceuticals currently used for renal evaluation are labeled with γ-emitting radionuclides γ -Radiation penetrates tissue as do x-rays and is detected by the γ-camera Current technology allows a continuous dynamic observation of the radioactivity accumulating in the urinary system Accumulation in the kidney of any of these chemicals is dependent initially upon renal blood flow, which is sufficiently large that the kidneys are seen as well-defined images with relatively little labeling of surrounding structures Thus, isotopic studies can be used to determine vascularity in any renal mass lesion A "cold" area with little radioactivity suggests a lack of vascularity and, if spherical, a cyst An area of high vascularity suggests a vascular tumor, usually a neoplasm Vascular tumors often demonstrate greatest uptake of radioactivity at a time which differs from that of the uninvolved renal cortex In the presence of neoplastic disease, the surrounding renal cortex may show reduced blood flow due to the local pressure of the tumor or to invasion of vascular structures Simple cysts tend to cause discrete spherical defects without other disturbance of renal cortical blood flow.
Renal Evaluation with Radioisotopes Scintiphotography also provides an opportunity to determine the presence of regional renal ischemia causing renal vascular hypertension The site of regional renal ischemia often may be defined, rather than just comparing one entire kidney to the other Scintiphotography is also an excellent tool for evaluating the success of vascular and ureteral anastomoses in the period immediately following transplantation In evaluation of renal trauma, radioisotopic studies are useful in the diagnosis of extrarenal hematoma, renal lacerations, reduction of renal function secondary to contusion, or urine extravasation Lastly, radioisotopes may be useful in obstructive uropathy and may give sufficient structural delineation to obviate the need for retrograde urography.
Ultrasound Evaluation of the Urinary System • Ultrasonic technics are increasingly being used to evaluate urinary system disease Much of the information obtained is purely anatomic, but the technic has the advantage that visualization does not depend on function Nevertheless, some functional information can be inferred, especially in the fetus, in whom the kidneys can be identified with certainty after about 20 wk gestation, permitting measurement of urine production rate by serial estimations of the bladder volume Fetal hydronephrosis, polycystic kidney, and bladder neck obstruction have also been detected In the neonatal period, ultrasound should be the first-choice technic for investigating abdominal masses, for the results may be 95 to 98% accurate • Ultrasound is extremely accurate in differentiating solid from cystic masses in patients of all ages Since ultrasound examinations are innocuous, they are also useful for the follow-up of known lesions, either without treatment—such as cysts incidentally detected—or after treatment for hydronephrosis or calculus This is especially the case in younger patients, in whom repeated radiographic examination is best avoided In transplanted kidneys, ultrasound has been used to detect and follow the progression of perinephric fluid collections Recent developments in ultrasound suggest the possibility of estimating blood flow in the kidney.
Renal Biopsy • There are four reasons for performing renal biopsies: (1) to help establish a histologic diagnosis; (2) to help estimate prognosis and the potential reversibility or progression of the renal lesion; (3) to estimate the value of therapeutic modalities; and (4) to determine the natural history of renal diseases. The only absolute contraindication to a biopsy is an uncontrollable bleeding disorder. The biopsy of a solitary kidney is a relative contraindication to be weighed against the need for information. Biopsies of a single, functioning, transplanted kidney are done frequently to diagnose and study possible graft rejections. Conditions associated with an increased morbidity following biopsy are deemed relative contraindications; these include renal tumors, large renal cysts, hydronephrosis, perinephric abscesses, severe reduction in blood or plasma volume, severe hypertension, and advanced renal failure with symptoms of uremia. • There are two biopsy technics, open and percutaneous; the percutaneous tech-nic is most common. The open surgical method is rarely necessary—only when the percutaneous method has been unsuccessful or when direct visual control of the biopsy is deemed critical. For the percutaneous technic the patient is sedated, and the kidney is visualized by radiographic or ultrasonic technics. With the patient in the prone position and following local anesthesia of the overlying skin and muscles of the back, the biopsy needle is inserted and tissue is obtained for light, electron, and immunofluorescent microscopy.
Oblique views to determine whether calcifications are intra- or extrarenal. (a) A rounded calcification is seen overlying the left kidney in the AP plain film, (b) In the oblique plain film, the calcification is in the same position within the renal shadow and is, therefore, a renal calculus, (c) A rounded calcification is seen over the right renal shadow, (d) An oblique film after contrast shows that the calcification lies outside the kidney. It was later confirmed to be a gall stone
Normal IVU. Full length 15min film. Note that the bladder is well opacified. The whole of the right ureter and part of the left ureter are seen. Often, only a portion of the ureter is visualized owing to peristalsis emptying certain sections. The bladder outline is reasonably smooth. The roof of the bladder shows a shallow indentation from the uterus.
Large calcified calculus in the pelvis of the kidney obscured by contrast medium. Since the contrast medium and the calculus have the same radiographic density, the calculus is hidden by the contrast medium.
Renal mass. A renal cyst (arrows) has caused a bulge on the lateral aspect of the kidney with splaying of the calices.
The calices. (a) Normal calices. Each calix is 'cup-shaped', (b) Many of the calices are clubbed. There is scarring of the parenchyma of the upper half of the kidney indicating that the diagnosis is chronic pyelonephritis, (c) All the calices are dilated, the dilatation of the collecting system extending down to the point of obstruction (arrow), in this case owing to a malignant retroperitoneal lymph node
At ultrasound, the kidneys should be smooth in outline. The parenchyma surrounds a central echodense region, known as the central echo complex (also called the renal sinus), consisting of the pelvicaliceal system, together with surrounding fat and renal blood vessels. In most instances, the normal pelvicaliceal system is not separately visualized. The renal cortex generates homogeneous echoes which are less intense than those of the adjacent liver or spleen and the renal pyramids are seen as triangular sonolucent areas adjacent to the renal sinus. During the first two months of life, cortical echoes are relatively more prominent and the renal pyramids are strikingly sonolucent. Normal renal ultrasound The normal adult renal length, measured by ultrasound, is 9-12cm. These figures are lower than those for renal size measured by IVU, because there is no swelling from the action of contrast medium and there is no magnification of the image.Normal ureters are not usually visualized. The urinary bladder should be examined in the distended state: the walls should be sharply defined and barely perceptible.
CT and MRIComputed tomography is used for specific indications, often after IVU or ultrasound have identified a problem.Like ultrasound, CT can characterize masses and it showsthe retroperitoneal space. It is an extremely sensitive method of detecting calculi andI is also useful when assessing trauma or infarction. The technique is virtually the same as for standard abdominal and pelvic CT, except that sections of the kidneys are usually performed both before and after intravenous contrast medium has been given.Magnetic resonance imaging gives similar information to CT, with a few specific advantages, but it has several disadvantages and is only used in selected circumstances, e.g. demonstrating renal artery stenosis and inferior vena caval extension of renal tumours.
Normal CTThe basic principles of interpretation are the same as for IVU. The renal parenchyma should have a smooth outline and opacify uniformly after intravenous contrast administration, although early images may show opacification of the cortex before medullary opacification has had time to occur. The pelvicaliceal system should show cupped calices with uniform width of renal parenchyma from calix to renal edge, and the fat that surrounds the pelvicaliceal system should be clearly visualized. The ureters are seen in cross-section as dots lying on the psoas muscles. They will not necessarily be seen at all levels because peristalsis obliterates the lumen intermittently. The bladder has a smooth outline contrasted against the pelvic fat; its wall is thin and of reasonably uniform diameter. Contrast opacification of the urine in the bladder is variable depending on how much contrast has reached the bladder. The contrast medium is heavier than urine and therefore, the dependent portion is usually more densely opacified.
Normal CT of kidneys and bladder, (a), (b) Adjacent sections, (b) 1 cm higher than (a), showing uniform opacification of parenchyma with well-defined cortical edge. The pelvicaliceal system, which is densely opacified, is surrounded by fat. The renal veins are well shown on the higher section, (c) (not present) Section through the level of the ureters (arrows) after contrast has been given, (d) Section through opacified bladder in a male patient shows that the bladder wall is too thin to be seen. Note the layering of contrast medium, (e) Section through bladder without contrast opacification. The bladder wall can be identified as a thin line. A, aorta; I, inferior vena cava; K, kidney; P, pelvis; RV, renal vein; Sp, spine.
Radionuclide examination • There are two main radionuclide techniques for studying the kidneys: • The renogram which measures renal function. Scans of renal morphology (DMSA scan). The advent of CT and ultrasound has reduced the need for such scans. They are now used mainly for evaluating renal scanning.
Renogram If substances which pass into the urine are labelled with a radionuclide and injected intravenously, their passage through the kidney can be observed with a gamma camera. The two agents of choice are "«Тс DTPA (diethylene triamine pentacetic acid) and ^mjc MAG-3 (mercaptoacetyl triglycine). DTPA is filtered by the glomeruli and not absorbed or secreted by the tubules, whereas MAG-3 is both filtered by the glomeruli and secreted by the tubules. The gamma camera is positioned posteriorly over the kidneys and a rapid injection of the radiopharmaceutical is given. Early images show the major blood vessels and both kidneys. Subsequently, activity is seen in the renal parenchyma and by 5min the collecting systems should be visible. Serial images over 20min show progressive excretion and clearance of activity from the kidneys. Quantitative assessment with a computer enables a renogram curve tobe produced and the relative function of each kidney calculated. The main indications for a renogram are: • measurement of relative renal function in each kidney -this may help the surgeon decide between nephrectomy ormore conservative surgery; • investigation of urinary tract obstruction, particularlypelviureteric junction obstruction; • investigation of renal transplants
Right kidney Minutes after injection 4 12 The renogram curve. a)Vascular phase. b) Filtration phase, (c) Excretion phase, (d)
Retrograde and antegrade pyelographyThe techniques of retrograde and antegrade pyelography (the term pyelography means demonstrating the pelvical-iceal system and ureters) involve direct injection of contrast material into the pelvicaliceal system or ureters through catheters placed via cystoscopy (retrograde pyelography) or percutaneously into the kidney via the loin (antegrade pyelography). The indications are limited to those situations where the information cannot be achieved by less invasive means, for example in those few cases of hydronephrosis where further information about the level and nature of obstruction is required.
Plain film showing a calcified staghorn calculus in each kidney.
Ultrasound of stone in right kidney. The stone (arrow) appears as a bright echo. Note the acoustic shadow behind the stone (double headed arrow).
Nephrocalcinosis. There are numerous calcifications in the pyramids of both kidneys (the left kidney is not illustrated). Ureteric obstruction. The pelvicaliceal system and ureter are dilated down to the level of the obstructing pathology (arrow), in this instance a small calculus
Acute ureteric obstruction from a stone in the lower end of the left ureter, (a) A film taken 30 min after the injection of contrast medium. There is obvious delay in the appearance of the pyelogram on the left. The left kidney shows a very dense nephrogram which is characteristic of acute ureteric obstruction, (b) A film taken 23 h later shows opacification of the obstructed collecting system down to the obstructing calculus (arrow).
Dilatation of the pelvicaliceal system, (a) Longitudinal ultrasound scan of right kidney showing spreading of the central echo complex of the dilated collecting system (arrows), (b) Here the dilatation of the calices is greater (arrows), (c) In this image from a patient with pelviureteric obstruction, the dilated calices resemble cysts, (d) CT scan after contrast showing a dilated renal pelvis (asterisk). The vertical arrow points to a small amount of contrast pooling in a dependent calix. Note the normal left ureter (horizontal arrow).
Renal pseudotumour (arrows) which was subsequently shown to be normal renal cortical tissue.
Ultrasound in renal masses, (a) Cyst (C) showing sharp walls and no echoes arising within the cyst. Note the acoustic enhancement behind the cyst, (b) Tumour showing echoes within a solid mass (M). (c) Complex mass due to cystic renal cell carcinoma. The arrows point to the edge of the mass. Note the thick septa within the mass, (d) Angiomyolipoma. This incidental finding shows the typical appearance of a small echogenic mass (arrow).
Computed tomography (contrast-enhanced) in renal masses, (a) Cyst in left kidney (C) showing a well-defined edge, imperceptible wall and uniform water density. The cyst shows no enhancement. It was an incidental finding, (b) Renal cell carcinoma. The mass (arrows) is not clearly demarcated from the adjacent kidney and shows substantial enhancement. (c) Angiomyolipoma with a small mass (arrow) of fat density.
Staging renal carcinoma, (a) CT scan showing a large mass (M) in the left kidney from renal cell carcinoma and a greatly enlarged lymph node (arrows) in the left paraaortic area. This node contained metastatic tumour cells, (b) Coronal MRI scan showing a huge left renal carcinoma (M) with tumour extending into the inferior vena cava (IVC) via the left renal vein. The caval extension of tumour (*) extends to the top of the IVC. (c) Axial MRI scan showing the IVC extension of tumour (arrows). Normally, the IVC is seen as a signal void.
Renal abscess, (a) Ultrasound scan showing a complex mass (arrows) in the right kidney, (b) CT scan in a different patient showing encapsulated fluid collection in the lower pole of the right kidney (arrows). D, diaphragm; L, liver; LK, left kidney; RK, right kidney; Sp, spleen.
Perinephric abscess. CT scan showing a rounded loculation of fluid and gas in the left perinephric space (arrows).
Renal trauma, (a) The lower pole of the kidney has been ruptured and a pool of extravasated contrast can be seen, (b) CT scan showing extensive haematoma (arrows) surrounding a fragmented left kidney (K)
Horseshoe kidneys, (a) The two kidneys are fused at their lower poles. The striking feature is the alteration in the axis of the kidneys: the lower calices are closer to the spine than the upper calices. The kidneys are rotated so that their pelves point forward and the lower calices point medially. The medial aspects of the lower poles cannot be identified, (b) CT scan of different patient, following i.v. contrast enhancement, showing fusion of the lower poles of the kidneys. K, kidney.
Bladder neoplasm, (a) There is a large filling defect in the left side of the bladder from a transitional cell carcinoma. Note the obstructive dilatation of the left ureter, (b) Ultrasound scan from a different patient showing a large tumour (T) within the bladder.
CT scan of carcinoma of bladder, showing an extensive tumour (T) involving the bladder wall but still confined to the bladder.
Bladder diverticula. Cystogram showing numerous outpouchings from the bladder with a very large diverticulum projecting to the left.
Prostatic enlargement. The bladder base is lifted up and shows an impression from the enlarged prostate (arrows). The ureters are tortuous and enter the bladder horizontally. A balloon catheter is in the bladder.
Prostate carcinoma shown by transrectal ultrasound. T, tumour. Carcinoma of the prostate. CT scan showing massively enlarged prostate (P) indenting the bladder. The tumour has spread to involve pelvic lymph nodes. A huge lymph node mass is seen (L). B, bladder; C, colon.
Small bowl Anterior abdominal wall Prostate carcinoma (T) invading lower part of bladder, shown on MRI scan (T1-weighted sagittal section).
Prostatic calcification. Numerous calculi just above the pubic symphysis are present in the prostate.
Urethral stricture. An ascending urethrogram showing a stricture in the penile urethra (arrow). The patient had gonorrhoea.
MRI of seminoma (arrow) in right testis. The two testes are well demonstrated. The high signal adjacent to both testes is normal fluid between the layers of the tunica vaginalis.
Normal uterus and vagina.Longitudinal section. The central echo of uterus (U) corresponds to the endometrial cavity; the uterus itself has a homogeneous echo texture; V, vagina; B, bladder.