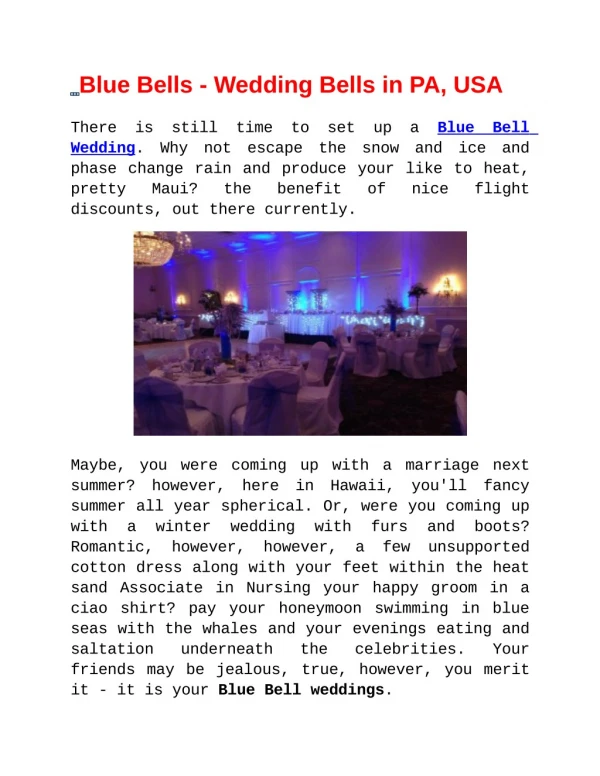
Bells Palsy
Bells Palsy. Aetiology . Most cases unknown Most likely cause is viral. Incidence. Commonest in age group 10-40yrs 20 cases per 100,000 people. Examination. Differentiate between upper and lower motor neurone lesion

Bells Palsy
E N D
Presentation Transcript
Aetiology • Most cases unknown • Most likely cause is viral
Incidence • Commonest in age group 10-40yrs • 20 cases per 100,000 people
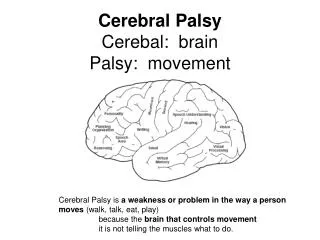
Examination • Differentiate between upper and lower motor neurone lesion • UML: frontalis is spared allowing normal furrowing of brow and eye blinking • LML: all muscles of facial expression are affected
Examination continued • Check no other cranial nerves involved (BP is an isolated VII lesion) • Look for a painful rash over the ears (Ramsay Hunt caused by H zoster)
Red flags which may necessitate referral • Bilateral BP • Recurrent BP • Association with rash elsewhere or with feeling generally unwell (sarcoid or Lyme disease) • Previous episode which might have been demyelination • ?SOL
Treatment • Prednislone 1mg/kg up to 80mg max per day tailing off in second week (reduces oedema) • Aciclovir 800mg 5x daily for 5days given within first 72hrs (prevents viral replication) • Consider tape/eye pad so patient can sleep • Consider prescription for artificial tears • Reassure patient that he hasn’t had a CVA
Follow up • 2/3rds of patients have spontaneous recovery • 85% show improvement in the first 3/52 • 15% show some improvement in 3-6/12 • Refer all cases to ENT after initiating Rx • Consider referral to eye specialist for tarsorrhaphy for those patients who have failed to make a complete recovery