Hepatitis B Virus infection
Hepatitis B Virus infection. Ermias D. (MD). History. Krugman et al (1967) – serum hepatitis/ HB Blumberg – Au Ag; (1976 Noble winner) Prince – SH Ag … HBsAg Opened up for rigorous investigations. Ethiopian epidemiology.


Hepatitis B Virus infection
E N D
Presentation Transcript
Hepatitis B Virus infection Ermias D. (MD)
History • Krugman et al (1967) – serum hepatitis/ HB • Blumberg – Au Ag; (1976 Noble winner) • Prince – SH Ag … HBsAg Opened up for rigorous investigations
Ethiopian epidemiology • E Tsega – serologic survey in 500 individuals from 5 regions • 6.2% HBsAg, • 42% overall viral markers, • increasing pattern anti HBe and decreasing HBeAg with age • 3 individuals with delta Ab • Arsi region among 20-24 yrs – 80% • H. Kefenie – among AA hospital personnel's (432) • HBsAg 9.02% • antiHBs 46.25% • antiHBc 73.6% • at least one marker 76.38% • A. Abebe - seroepidemiology in AA • HBsAg 7% • HBeAg 23% • increasing with age any marker 70% (40-49yrs) • Gondar 14.4% --- 8.2% (blood donors) • Review article (E. Tsega) - HBsAg 8-12%, over all markers 70 -79%
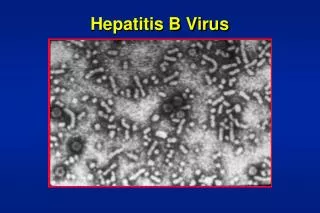
virology • Hepadnaviridae – hepatotrophic DNA virus • Small amount in kidney, pancreas, mononuclear cells • Infected cells produce two distinct subviral lipoproteins – HBsAg (spheres and filamentous forms) • Viral structure
40-42nm Outer lipoprotein Envelope (3 Surface Ag, glycoprotein) Core, viral genome DNA 3.2kb polymerase
8 subtypes group reactive and subtype Ag – a, d or y, w or r
Genes and proteins • preS-S gene • S - Major (HBsAg), • preS2 – middle (M), • PreS1 - large (L) – binding, assembly, release • preC-C • HBcAg – target of immune response • HBeAg – marker of active replication • P region – viral polymerase – DNA synthesis, RNA encapsidation • X gene – gene expression, vivo replication, spread
Viral replication cycle • Fusion • Core presentation to cytosol – - then nucleus • DNA – cccDNA • RNA transcription (host RNApolymerase II) • Pass to cytoplasm • Translation of envelop, core, polymerase, x, preC • Assembly (including single RNA) • Sequential DNA synthesis (first from RNA by RT, the second from the first synthesized DNA) • Recycle from the cytoplasm with in the cell itself or bud out and infect other cells
pathogenesis • Viral replication – not cytotoxic • Many carriers - asymptomatic • Host immune response – hepatocellular injury • Pt with immune defects – minimal injury • In acute self limited disease – strong T cell response – MHC II CD4 T, MHC I CD8 T • Cytotoxic T response against - core, polymerase, envelope proteins (central roll in viral clearance) • Helper T against – C and P proteins • Chronic infection – attenuated T cell response • Virogous Ab response
Conti… • Transgenic mice - tolerant to HBV proteins and there is no significant liver injury • Administration of cytotoxic T cell from syngeneic animals – acute liver injury • Few hepatocytes are directly killed by the cyt. T cell and their target • Secondary antigen nonspecific inflammatory responses, cytotoxic by products of inflammatory response, TNF, free radicals proteases, other immune cells • TNF and IFN have antiviral effect with out killing target cells – important for viral clearance • Cytokine release by un related hepatic infections has similar effect
Natural history • Primary infection is mostly asymptomatic • Mostly self limiting with viral clearance and lasting immunity • 5% persistent infection – viral replication and viremia continues • Persistent infection: • Symptomatic (chronic) – abnormal liver function and histology • Asymptomatic (carriers) – normal serum amino transferase and histology • 20% chronic – fibrosis and regenerative nodules (cirrhosis)
Viral DNA HBsAg HBeAg Anti HBc ALT AntiHBe AntiHBs Viral DNA HBsAg Anti HBc HBeAg ALT AntiHBe ALT
Hepatocellular carcinoma • 100 times risk in chronically infected patients • HBsAg and HBeAg positive have higher risk • Even anti HBe antibody carriers have risk • Molecular mechanism incompletely understood • Twice a year screening with serum α FP or liver sonography or both • α-FP low positive predictive value (9-30)
Hepatitis D • Defective RNA virus • Requires host polymerase II for replication • Require the helper function of HBV to cause liver injury • Endemic in HB infected • Duration of infection cannot out last HBV infection • Transmission – close personal, percutaneous • Simultaneous co infection • Chronic infection – <5%, • fulminant failure 1%, • mostly complete recovery • Super infection in HBsAg positives – • fulminant failure 5% • 80-90% chronic infection and rapid cirrhosis and HCC
Manifestation • Similar to other viral hepatitis • IP 4-12 weeks • Prodromal symptoms – acute viral infection (1-2 wks) • Clinical Jaundice, nausea, vomiting, alteration in olifaction and taste. Dark urine, clay like stool • Icterus, fever, RUQ tenderness • Recovery phase liver enlargement and functional abnormality may persist (2-12 wks) • In HDV infection - 90% asymptomatic, similar sx • HDV Ag 20%, HDV RNA 90% • elevated transaminases
Extrahepatic manifestations • Immune complex mediated • Serum sickness like syndrome (acute HB) • Glomerulonephritis (hypocomplementemic) with nephritic syndrome • Polyarteritis nodosa • Essential mixed cryoglobulinemia (HCV) • Pulmonary hemorrhage, vasculitis • Acute pericarditis, polyserositis • Henoch-Schonlein purpura
Diagnosis Thank you
Case discussion • 38 yrs old male • Bilateral leg swelling for 5 years
History • Bilateral leg swelling since 4 wks following an acute episode of diarrheal disease • The diarrhea was watery moderate in amount and subsided after four days, pt took norfloxacillin • He has the leg swelling for the last five yrs waxing and wanning in intensity • Gets worse with stressful situations, hot whether, and anorexia (poor feeding) • Long standing dyspeptic sx – take anti acids, PPI, H2B • Infrequent use of paracitamol, diclofenac for migraine • Bowel habit is often constant with once per day, no stool color changes • 2 pack yrs of smoking before 10 yrs • Nutritional hx - 3meals/day small; • No cardiac sx or illness before • No urinary abnormality
p/E • V/s in the normal ranges • Wt 55kg • Pedal and pretibial gross pitting edema
Lab data • 14/11/01 • Hgb 17.5 • Total serum protien – 6 (LLN 6.2) • Alb - ?? • Electrophoresis a/g 1.42 (normal) • UA, liver enzymes, renal function, FBS, abdominal US --- normal
Dec. 2004 • Hgb – 17.1 • ESR – 0 • TFT – wnl • Doppler of the leg vessels – normal • ANA positive, LE body negative • Cl- 118 • Abdominal US, UA, liver enzymes, RFT, Na, K - wnl
Wbc 8700 L% 11 • Hgb – 19.3 MCV – 87 • UA protein +, repeat – negative for protein • TSP 3.4, albumin 3.1 • a/g – 1.31(1.39 – 2.23) • ESR – 3 • Cl- 117, CO2 13(21-32) • Lipid profile, liver enzymes, PT, Na, K, RFT, - WNL • Stool 3X negative • H.pylori serology - Negative
discussion • Protein lossing enteropathy • Underlying cause • ?? PUD • Long standing dyspepsia • Polycythemia • Elevated serum Cl- • Low total protein and albumin