Download

1 / 38
450 likes | 1.02k Vues
Pyrexia of unknown origin and Fever in returning traveller. Dr Richard Drew Research Fellow Dept Clinical Microbiology. What is PUO. Originally defined in 1961 by Petersdorf and Beeson Fever >38.3C on 3 or more occasions Fever for more then three weeks

E N D
Pyrexia of unknown origin and Fever in returning traveller Dr Richard Drew Research Fellow Dept Clinical Microbiology
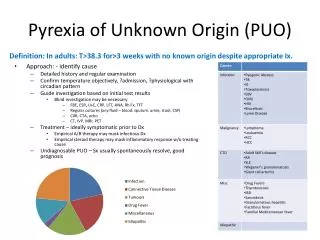
What is PUO • Originally defined in 1961 by Petersdorf and Beeson • Fever >38.3C on 3 or more occasions • Fever for more then three weeks • Uncertain diagnosis after one week in hospital • Very rare nowadays in hospital
How to solve the problem • History • Physical examination • Blood tests • Imaging • Endoscopy and tumour markers
Aetiology • Infections • Malignancies • Connective tissue disorders
History • Fever: Pattern, periodicity, how was it measured • Associated symptoms such as sweating, vomiting, headaches etc. • Target specific organ systems if patient has problems in that system • Past med and surg hx. NB prostheses in situ • Medications/ vaccines • Family hx of hereditary diseases, connective tissue disorders or recent illnesses (TB/ AIDS) • Sexual history • Occupation, pets, travel
Examination • Full physical examination is needed. Should be very detailed and review all systems. • For exams make sure to examine: • Hands for stigmata of infective endocarditis • Retinal exam for candidiasis or toxoplasmosis • Teeth (infective endo or abscess) • Lymphadenopathy (AIDS or chronic infections) • Hepatosplenomegaly (Lymphoma/leukaemia) • Breast/testicular exams • Any sore joints
Infections • Tuberculosis • HIV/AIDS • Abscess • Osteomyelitis • Infective Endocarditis
tuberculosis • Classical prevention is fever, haemoptysis, cough, weight loss and night sweats • Risk Factors: Alcoholic, homeless, drug abuser, immigrant • On exam can have pleural rub, pleural effusion and lymphadenopathy. Check if BCG vaccinated • Do Mantoux test, CXR and sputum for AFB and TB culture. • Treatment is 4 drug regimen (RIPE) and inform public health • Isolate patient for 2 weeks in negative pressure room and wear FFP3 masks • Always consider in differential of patient with cough and PUO
HIV/ AIDS • No classical presentation. Can present with fever, weight loss, sweats, lymphadenopathy or with opportunistic infection • Hx: Sexual contacts, Birthplace, Maternal hx if child, Exposure events, occupation • O/E Full exam. Lymph nodes and spleen • Ix: HIV antibody test and HIV viral load, CD4 count • Mx: Refer to ID team. HAART
Osteomyelitis • Infection of the bone • Spontaneous osteomyelitis is rare apart from in Sickle cell disease patients • Consider if prosthesis is in situ or if there is a history of preceeding compound fractures • FBC, ESR, Imaging of joint, bone biopsy • Mx: Targeted antimicrobial therapy and prosthesis removal
Non-infectious causes • Malignancies • Lymphoma • Leukaemia • Solid organ tumours • Connective tissue disorders • Still’s disease • Giant cell arteritis
Malignancies • Leukaemia/Lymphoma • Hx: fever, sweats, weight loss, fatigue • O/E, Lymph nodes, hepatosplenomegaly • Ix: Bone Marrow aspirate, blood smear, FBC • Mx: Chemotherapy+/- Bone Marrow transplant • Solid Organ tumours • Target the particular organ you feel is involved. • Connective tissue disorders • Hx: Fatigue, unexplained rashes, arthralgia, myalgia • O/E arthralgia, uveitis, Raynaud’s phenomenon • Ix: ESR • Mx: Steroids, NSAIDs
Investigations • Basic tests • FBC: WCC, blood smear, • bone marrow aspirate • ESR, CRP: Non-specific markers of inflammation • CXR, Mammogram, Pap smear if relevant, Mantoux, • Micro: Blood cultures (3 sets) • Other tests to consider • The clue is in the history as to what tests are needed • HIV test, viral and bacterial serology • CT thorax/ abdomen • Tumour markers • Echocardiogram
Management • Determine if critically ill. If not can hold off on antibiotics • Don’t feel need to just treat a temperature • Clue is in the history and the exam and then order relevant tests. Do not send random serological tests off. Often these will cause more trouble then you want!!!
Returning Traveller • Very common problem • Geosentinel data review (Clin Infect Dis. 2007) of 25,000 ill returning travellers • 28% had fever and 26% of these needed admission • Malaria was the most common diagnosis • Considerable geographical variation • 17% had vaccine preventable diseases • Will discuss methods of diagnosing the condition and not each disease in detail
History • Crucial. Will help to narrow down possible list of diseases. • Don’t always get distracted by history of recent travel. May be more common diagnosis • Exposure: Duration, exact location, urban/rural, type of accomadation • Timing: Consider incubation period and onset of symtoms. 66% of dengue presents within one week of return. 34% of hepA presents within 6 weeks • Food history is important • Sexual history is important • Vaccine history
Examination • Full examination as per previous PUO talk • Need to consider the risk of a transmissible organism • Consider isolating patient until diagnosis is known • Critical if considering a viral haemorrhagic fever • Signs that should trigger full resuscitation and precautions • Bleeding symptoms, respiratory symptoms • Hypotension • Signs of meningitis or raised intracranial pressure
Evaluation • Thick and Thin smears for malaria • FBC: Look for raised white cells • Renal profile: Dehydration, renal failure • Liver profile: hepatitis • Coagulation screen • CXR if respiratory symptoms
Top 5 diagnoses (Geosentinel) • Malaria • Dengue Fever • EBV/CMV mononucleosis • Rickettsia • Typhoid
26yr IVDA from Dublin Self discharged twice before from hospital having been admitted with fever Reports to have had fever and night sweats for about 4 weeks. Has lost 2 stone in 3 months Some visible skin sores and needle marks Pulse 110bpm, Temp 36C, BP 100/60 Differential diagnosis History Examination Lab tests at 3am Lab tests the following day Infection Control Management Public Health Clinical Case 1
Returning GOAL worker. 28 yr male. Worked for 12 months in rural clinic in Rwanda 2 episodes of infectious diarrhoea while there Presented to ED three days after coming home Looks very unwell. Non blanching skin rash Differential diagnosis History Examination Lab tests at 3am Lab tests the following day Infection Control Management Public Health Clinical Case 2