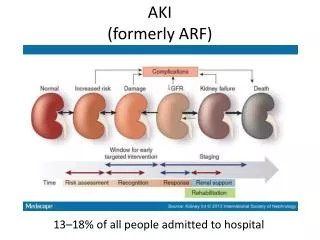
AKI
AKI. Objectives. Definition of AKI Understand the epidemiology of AKI and its association with mortality Understand the limitations of GFR assessment during AKI Understand how to use diagnostic methods available to identify reversible causes Reinforce the importance of AKI prevention.

AKI
E N D
Presentation Transcript
Objectives • Definition of AKI • Understand the epidemiology of AKI and its association with mortality • Understand the limitations of GFR assessment during AKI • Understand how to use diagnostic methods available to identify reversible causes • Reinforce the importance of AKI prevention
AKI Mimics • A rise in the creatinine level does not necessarily correlate with AKI • Result of medications (cimetidine, trimethoprim) that inhibit the kidney’s tubular secretion • A rise in the BUN level can also occur without renal injury • GI or mucosal bleeding • Steroid use • Protein loading
Acute or Chronic? • Findings suggestive of chronic renal failure: • Documented chronic increase in serum creatinine • Small kidneys on renal imaging • Findings c/w osteitis fibrosa cystica on x-ray • Relatively asymptomatic at very high levels of BUN and creatinine
Urine Volume • Urine flow rate • Oliguria • Defined as < 400 ml/day or < 0.5 mg/kg/hr • Minimal amount of urine needed to clear waste products in 24 hr is 400-500 ml • Non-oliguria • Studies range from 20 - 60% of patients • Anuria (<100 ml/day) – suggests complete obstruction, complete lack of blood flow into kidneys, and cortical necrosis
Using FeNa FeNa = (UNa x Pcreat)/(Ucreat x PNa) x 100% In Nonoliguric states • FeNa < 1% in pre-renal azotemia • FeNa > 3% in oliguric ATN Miller TR, et al. Ann Int Med 1978; 89: 47-50.
FeUrea • The measurement of the fractional excretion of urea (FeUrea) may be useful in patients with AKI • ATN: FeUrea 50 – 65% • Pre-renal: FeUrea usually <35% • Inconsistent results have been reported • FeUrea should not be used in isolation (should be used together with clinical history and other laboratory tests to differentiate between pre-renal and ATN)
Renal Ultrasound • 98% sensitive for obstruction • Also useful for size, echogenicity, cortical thickness • Small kidneys (chronic severe renal failure) • Enlarged kidneys (ADPKD, HIV, amyloid, acute GN, DM, malignancy, renal vein thrombosis)
Size Matters • Remember, length is only one dimension • Median adult renal length • Left = 11.2 cm • Right = 10.9 cm • Standard deviation 1.2 – 1.3 cm • Parenchymal thickness usually 1.5 – 1.6 cm • Renal size difference typically <2 cm • Echogenicity is ≤ liver
Nuclear Imaging • Dynamic radionuclide scans assess renal excretory function and utilize either technetium 99mTc-diethylenetriamine pentaacetic acid (DTPA) or 99mTc-mercaptotriglycylglycine (MAG-3) as radiotracers. • Used to assess renal blood flow and tubular function • Differentiates between obstructive versus non-obstructive causes of hydronephrosis • DMSA renal scan • 99mTc–dimercaptosuccinic acid (DMSA) is used as the radiotracer • Used to assess whether a suspected renal lesion contains normal-functioning nephrons and/or the differential function of the two kidneys; also detects renal scarring
Nuclear Imaging • DMSA renal scan • 99mTc–dimercaptosuccinic acid (DMSA) is used as the radiotracer • Used to assess whether a suspected renal lesion contains normal-functioning nephrons and/or the differential function of the two kidneys; also detects renal scarring
Post-ATN Diuresis • Normal diuresis of retained fluids after recovery of renal function • Tubular dysfunction often persists after Cr drops and UOP increases • AVP resistance: unable to concentrate urine • Manifested by hypernatremia, low urine SG • Replace with D5W or oral water, titrate to [Na] • Electrolyte wasting (K, PO4, Mg, Ca)
Conclusions • AKI is a common inpatient complication • Associated with high mortality rate (up to 80%) • Timely evaluation and treatment of reversible causes is key to survival • Prevention is more effective than treatment of established AKI • RRT is supportive pending recovery of native renal function