Download
1 / 61
670 likes | 1.11k Vues
Traumatic Hemorrhagic Shock and Massive Transfusion Protocols in Children. Philip C. Spinella , MD. FCCM Associate Professor, Department of Pediatrics Critical Care Translational Research Program Director Washington University in St Louis. Epidemiology.

E N D
Traumatic Hemorrhagic Shock and Massive Transfusion Protocols in Children Philip C. Spinella, MD. FCCM Associate Professor, Department of Pediatrics Critical Care Translational Research Program Director Washington University in St Louis
Epidemiology • Trauma most common cause of death • Children > 1 year of age in US • Hemorrhage most common cause of preventable death • 66-80% of preventable deaths are from hemorrhage • Hemorrhagic death occurs fast – 6-12 hours • Prevention of early death from hemorrhage - important • Greatest Impact on Survival
Objective: Incidence, association with mortality • Shock and coagulopathy • Retrospective: Combat Support Hospitals • 744 children in Iraq and Afghanistan from 2002-2009 • Coagulopathy and Shock • INR ≥1.5 • Base deficit (BD) ≥6.
Coagulopathy 27% (202/744) of patients presented w/ coagulopathy
Shock 38.3% (285/744) of patients presented with early shock
Adjusted Analysis Table 3. Logistic regression results for in-hospital mortality Coagulopathy & shock, OR =3.8 (95% CI 2.0-7.4), (p<0.001)
Results • 707 patients from the derivation set and • 1101 patients in the validation set. Table 2. Multivariate Logistic Regression for Mortality INR, International Normalized Ratio
Results • Pediatric “BIG” score • (Base Deficit + (2.5xINR) + (15-GCS) • AUC for derivation and validation datasets • 0.89 (95% CI 0.83-0.95) • 0.89 (95% CI 0.87-0.92)
Grade V liver injury has a 76% mortality in academic Level 1 Trauma Centers
DCR • INDICATION: LIFE THREATENING INJURY
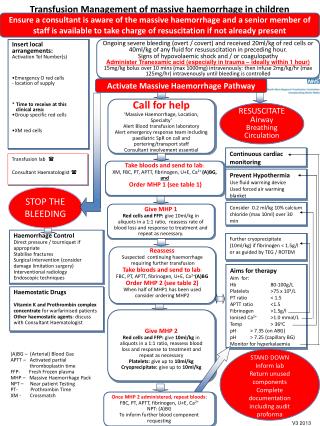
Massive Transfusion Protocol • MTP Principles • Rapid surgical control • Avoid overuse of crystalloids to minimize dilutional coagulopathy • Continuously monitor patient temperature • Avoid and treat hypothermia (use fluid warmer and Bair hugger if needed) • Avoid and treat acidosis as needed; (pH<7.2 treat with bicarbonate or THAM) • Treat low ionized calcium for hemostatic and hemodynamic effects Laboratory evaluation upon admission I stat: blood gas, lactate, Hb, ionized calcium and electrolytes, INR/PT. Laboratory: Type & Screen, CBC, Fibrinogen, TEG (if available) – STAT Laboratory Evaluation q hour until MTP stops I stat: blood gas, lactate, Hb, ionized calcium and electrolytes, INR/PT. Laboratory: CBC, Fibrinogen, TEG (if available) – STAT
Adjunctive Therapies • Fibrinogen concentrates • 30-50 mg/kg • Fibrinogen concentration or TEG based • Prothrombin complex concentrates • Factors II, IX, X • Factors II, VII, IX and X, Protein C and S – FDA IND • Anti-fibrinolytics • Tranexamic Acid (TXA) • rFVIIa
CRASH-2 Trial • Clinical Randomization of an Antifibrinolytic in Significant Hemorrhage (Lancet, 2010) • Prospective of 20,211 patients • Multicenter (270 Hospitals) • Multinational (40 Nations) • Randomized, Blinded, Placebo-controlled • One gram tranexamic acid over ten minutesfollowed by one gram tranexamic acid given over eight hours • Normal saline placebo
CRASH-2 Trial • Inclusion Criteria: • Adult Trauma victim • Systolic blood pressure less than 90 mmHg • Heart rate greater than 110 • Deemed to be at risk of significant hemorrhage
CRASH-2 Trial • Endpoints: • Primary: In-hospital death within four weeks of injury • Secondary • Vascular occlusive events • Surgical interventions • Blood Transfusions • Total units of blood transfused
CRASH-2 Trial- Results • Decreased mortality: • All-comers, 14.5% vs. 16.0% (p=0.0035) • Deaths from bleeding, 4.9% vs. 5.7% (p=0.0077)
CRASH-2 Trial- Results • Treatment ≤1 h from injury reduced risk of death due to bleeding • 5.3% in TXA vs 7.7% in placebo • RR 0.68, (95% CI 0.57–0.82), (p<0.0001) • Treatment from 1- 3 h also reduced risk of death due to bleeding • 4.8% vs. 6.1% • RR 0.79, (0.64–0.97) (p=0.03). • Treatment > 3 h increased the risk of death due to bleeding • 4.4% vs. 3.1%, • RR 1.44, (1.12–1.84), (p=0.004)
MATTERs Study • Military Application of Tranexamic Acid in Trauma Emergency Resuscitation (Arch Surg, 2012) • Retrospective, observational of: • 896 Combat-injured patients (both soldiers and nationals) presenting to Camp Bastion Surgical Hospital in Afghanistan • Requiring a minimum transfusion of one unit packed red blood cells
MATTERs Study • Endpoints: • Primary: 24-hour, 48-hour, and in-hospital mortality • Secondary: • Transfusion requirement • Correction of PT and PTT between admission and ICU • Thromboembolic events
MATTERs Study • Results (896 patients, 293 receiving TXA): • Greater injury severity in TXA-treated group • (ISS 25.2 vs. 22.5, p<0.001) • Greater transfusion requirement in TXA-treated group • (All products) • Decreased Mortality in TXA treated: • 48-hour (11.3 vs. 18.9%, p=0.004) • In-hospital (17.4 vs. 23.9%, p=0.030) • Reduction in hypocoagulability in TXA-treated group from ED to ICU
MATTERs Study • Thromboembolic events increased with TXA: • PE • (8 vs. 2, p=0.001) • DVT • (7 vs. 1, p=0.001)
Should TXA be used in Peds MTPs? • No evidence at all in children • Adult data appears supportive • Standard in Adult MTPs • Reasonable to add • Reasonable to wait for additional data
Fibrinogen Concentrates • Provide high amount of fibrinogen rapidly • Not frozen, rapidly reconstituted and given • High cost • No comparative data with cryoprecipitate in trauma patients
Goal Directed Hemostatic Resuscitation • Hemostatic Resuscitation = 1:1:1 • Goal directed hemostatic resuscitation • 1:1:1 that is tailored to patients needs
Thromboelastography (TEG) • Whole blood test • Plasma-platelet interaction • Patient temperature • Functional measurement of • Clot initiation, amplification, propagation, lysis • TEG system • Laboratory based • Point of care • Remote - networked
TEG Parameter Summary TEG Parameter Summary
Whole Blood Availability • Classic teaching is that Platelets stored at 4C are non functional • Current data indicates IMPROVED function • If whole blood can be stored for 10 days at 4C. • Improved hemostatic effects in vivo • Increase clinical utility significantly
Average ± SEM ADP-, collagen-, ASPI-, and TRAP-6-stimulated aggregation in WB stored at 4º C versus 22º C (p<0.001 for all four agonists by repeated measures ANOVA). Pidcoke,H.F., Pidcoke, Heather, Transfusion. 2013 Jan;53 Suppl 1:137S-49S.
Manno - Methods • Prospective double-blinded study • 161 children requiring cardiac surgery • Patients were randomized to • Warm FWB (< 6 hours at 20 degrees C) • Cold FWB (24 - 48 hours at 4-6 C) • Reconstituted whole blood (1:1:1) • (RBCs ≤ 5 days of storage, FFP, and platelets). Manno CS, et al. Blood 1991;77:930-6.
Manno - Results • Patient groups similar • Sex and Age • Surgical severity score • By pass and circulatory arrest time • # requiring circulatory arrest
Manno - Results ∞ cold vs recon § warm and cold vs recon Manno CS, et al. Blood 1991;77:930-6.
Warm FWB Benefits & Risks • Benefits • Less dilutionaleffect than components • Less anti-coagulants and preservatives1 • More functional fresh product 2 • No storage lesion (adverse effects) of RBC • Risks • Infectious, GVHD, WBC mediated 1 Spinella PC, J Trauma. 2009;66:S69-76 2 Manno CS. Blood 1991;77:930-6.
Cold Whole Blood Trials • Liver Transplant • Burn • Trauma
Case Example Intraoperative Hemorrhagic Shock • A 9 year old 20 kilogram male, who previously underwent a right nephrectomy and pulmonary resection for Wilmstumor, presented one year later with a new lesion in the right lobe of his liver
Case Example • The patient was taken to the operating room (OR) and a right hepatectomy was performed • Due to severe intra-operative bleeding the MT protocol was activated
Case Example • During the 4 hours that the MT protocol was activated, a total of 10 units RBCs, 14 units FFP, and 15 units of platelets were transfused. (20 kg child) • With EBL of over 4 liters no laboratory evidence of a metabolic acidosis or shock indicated by normal base deficit values
Case Example • Upon admission to the (ICU) • After receiving an intraoperative total of 13,100 milliliters (ml) of blood products • (8 blood volumes) • And 4,500 ml of normal saline • Patient had no physical evidence of pulmonary edema or anasarca.
Case Example • Patient had no physical evidence of pulmonary edema or anasarca. • PEEP of 5 with Fi02 30% • Extubated in AM