Soft Tissue Sarcoma
Soft Tissue Sarcoma. Craig Blum, M.D. Soft Tissue Sarcoma. Arise from embyronic mesoderm Ecoderm- skin Endoderm- guts Mesoderm- skeleton and muscles, connective tissue. Osteosarcoma Chondrosarcoma GIST Ewing Sarcoma. Fibrosarcoma Liposarcoma Rhabdomyosarcoma Epitheloid Sarcoma


Soft Tissue Sarcoma
E N D
Presentation Transcript
Soft Tissue Sarcoma Craig Blum, M.D.
Soft Tissue Sarcoma • Arise from embyronic mesoderm • Ecoderm- skin • Endoderm- guts • Mesoderm- skeleton and muscles, connective tissue
Osteosarcoma Chondrosarcoma GIST Ewing Sarcoma Fibrosarcoma Liposarcoma Rhabdomyosarcoma Epitheloid Sarcoma Desmoplastic small round cell tumor Histologic Types
Incidence • Rare tumors • 2007: • 9200 US • 3560 deaths • colon 112,000 • lung 214,000
Cause • Unclear: • Genetic factors: chromosomal abnormalities • Radiation: long latency • Chemical exposure: industrial agents • Lymphedema: **absite • lymphangiosarcomas
Classification • Best predictor of a sarcoma’s biologic aggressiveness / metastatic potential is GRADE • Cellularity, nuclear atypia, degree of necrosis, mitotic activity. • Subjectivity (40%)
Clinical • Asymptomatic mass • 38% large than 10cm at presentation • Imaging: • MRI versus CT • PET
Pearl • Few sarcomas metastasize to lymph nodes • Extremity Lung • Abdominal Liver then lung
Biopsy • <5 cm: excisional biopsy with clear margins • >5cm: incisional or core needle bx (CNB) • Don’t use FNA bc sample too small
Treatment • Surgical Tx is foundation of treatment of STS • LSS standard of care • Amputation reserved for cancers that involve major vessels, bones, nerves such that function would be compromised.
Surgical Management • Goal margin 1 -2 cm when possible. • Regional lymphadenectomy is NOT usually indicated bc only 2.6% sarcomas metastasize to LN • Rhabdomyosarcoma • Epitheloid sarcoma (CT of hands) • Clear cell sarcoma (tendons) • Synovial sarcoma • Vascular sarcoma
Radiation • Take home: • [prospective, randomized trails] demonstrated adjuvant radiotherapy helped prevent local recurrence in pts with high grade STS. • However, did not demonstrate improved overall survival. • [retrospective studies] <5cm (small) STS may be resected with negative margins alone.
Chemo • Take home: • “At present, given the uncertainty regarding its efficacy, postoperative adjuvant chemotherapy for treatment of STS is probably best employed in the context of appropriate clinical trials.” • Preop “theoretical advantages” but again, insufficient evidence for any survival benefit.
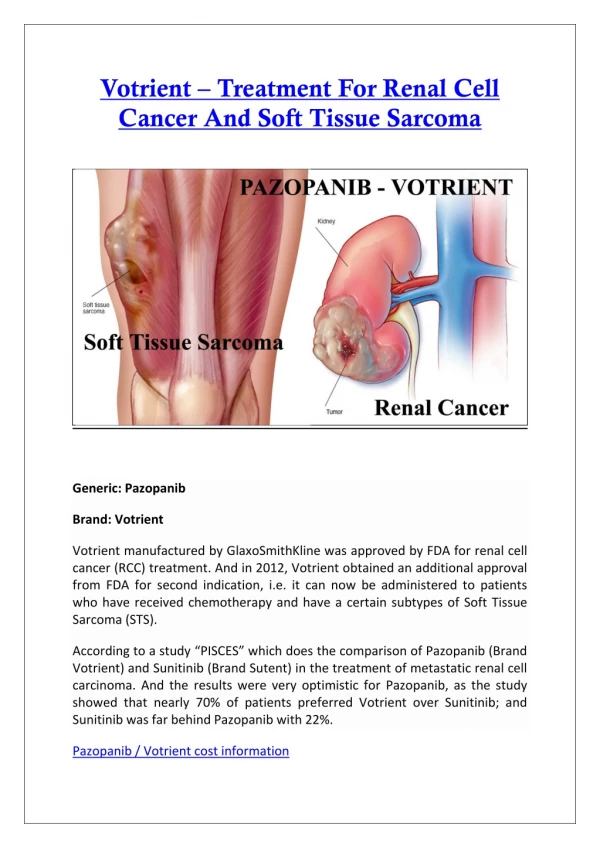
Targeted Therapy • Targeted tyrosine kinase receptor c-kit for treating GIST
Hyperthermic Isolated Limb Perfusion • Pts where LSS is not possible initially • May make it possible to resect with a negative margin. • Not well established in US
Metastatic Disease • Pulmonary mets are present in 20% of pts with trunk of extremity sarcomas. • Medically fit, no extrathoracic dx, mets resectable pulmonary metastasectomy. • MSKCC study
Rhabdomyosarcoma • most common soft tissue sarcoma in infants and children • head and neck; around the eyes -- 35-40% • GU tract -- 20% • extremities -- 15-20% • trunk -- 10-15%