Download
1 / 23
240 likes | 536 Vues
Septic arthritis Reşat ÖZARAS, MD, Prof. Infection Dept. rozaras@yahoo.com. SEPTIC ARTHRITIS. Infection of synovium and synovial fluid Seen in every ages Hip joint in children Knee in adults. }. frequent. ETIOLOGY. S. aureus → in every ages H. influenzae → 6 mo-5 years

E N D
Septic arthritisReşat ÖZARAS, MD, Prof. Infection Dept. rozaras@yahoo.com
SEPTIC ARTHRITIS • Infection of synovium and synovial fluid • Seen in every ages • Hip joint in children • Knee in adults } frequent
ETIOLOGY • S. aureus→in every ages • H. influenzae→6 mo-5 years • N. gonorrhoeae→ >10 years, adults (in Western populations) • Gram negative bacilli →Immune deficiency, urinary or intestinal invasive procedures, elderly people, renal failure, chronic joint disorders and diabetes
ETIOLOGY • S. epidermidis→Prosthetic joint • S. aureus/Pseudomonas →i.v. drug use • S. pneumoniae→Alcoholism, pneumonia, meningitis • L. monocytogenes→Immune deficiency • Atypical mycobacteria → Chronic infection
PATHOGENESIS • Hemotogenous spread • Spread through adjacent tissues • Direct inoculation(aspiration/arthrotomy) *Rheumatic diseases are underlying disorders for septic arthritis -Structural abnormalities in the joint -Steroid use (abnormal phagocytosis…) *DM, immune def, hematological diseases, trauma, systemic infections…
CLINICAL FEATURES • Usually, there is a history of recent trauma/infection • Frequently hip and knee joints • Sacroiliac joint is affected in brucellosis • Interphalangeal joints: human and animal bites • Fever, fatigue, anorexia, nausea… • Local findings of inflammation
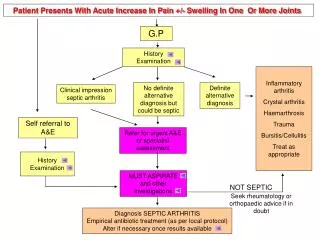
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS • Synovial fluid sampling: >50.000 leukocytes/ml (crystal arthropathies and RA) • Leukocytes <50.000/ml (Malignancy, steroid use) • Gram staining and culture • Gram-positive bacteria 60%, Gram-negative bacteria 40%
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS • Blood culture / urethral discharge culture • Yield rate of microorganism 70% • Antigen detection (S. pyogenes, S. pneumoniae, H. influenzae) • PCR (B. burgdorferi, N. gonorrhoeae) • Leukocytosis, ESR, and CRP increase
DIFFERENTIAL DIAGNOSIS • Rheumatic fever • Acute juvenile arthritis • RA, gout, reactive arthritis • Viral arthritis • Fungal arthritis • Tuberculous arthritis • Osteomyelitis • Cellulitis • Bleeding into the joint (hemarthrosis)
TREATMENT • <5 year-old: 2nd and 3rd generation cephalosporins • >5 year-old and adults: cefazolin, 2nd gen. cephalosporins • S. aureus→cefazolin/vancomycin • Adults: ciprofloxacin+rifampin • N. gonorrhoeae→cefriaxone, • Gram-negative bacilli→3rd gen. cephalosporin+ aminoglycoside
Gram-positive • Streptococcus, methicillin-sensitive staphylococcus • Cefazolin 3x2 gram, Sulbactam/ampicillin 4x2 gram • Meticillin-resistant staphylococcus • Vancomycin 2x1 gram • Gram-negative • Ceftriaxone 1x2 gram
TREATMENT • Parenteral tx: 5-7 days then switch to oral tx (2-4 weeks) • Gram-negative bacilli and S. aureus→ 3 weeks • Needle aspiration and irrigation →Septic arthritis needs intervention (emergency) ! • Hip joint septic arthritis →surgical drainage (Arthritis may disrupt the blood supply of the hip joint)
VIRAL ARTHRITIS • Usually begins suddenly • In developed countries, Parvovirus-B19, • In children, fever, headache, rash, fatigue • Polyarthralgia • Symmetrical joint pain
VIRAL ARTHRITIS • In adults, rubella can cause viral arthritis • Its rate decreases due to mass vaccination during childhood • Infection itself/ after immunization • It involves small joints
VIRAL ARTHRITIS • Diagnosis; clinical/serological and polymerase chain reaction (PCR) • It resolves spontaneously within 2 weeks, • In some (20%) female patients, arthritis may persist for 2 months • No erosion was seen on joints
Mycobacterial Arthritis • 10-11% of extrapulmonary TB is bone /joint TB • 1-3% of all TB cases • Incidence ↑( HIV prevalence↑) • In endemic regions, children and young adults; in other parts elderly and immunosuppressed ones. • Risk factors Low socioeconomical status, alcohol, i.v. drug use, immunosuppressive therapy, HIV infection, joint disorders…
Mycobacterial Arthritis • M. tuberculosis → chronic granulomatous monoarthritis • Hematogenous spread after primary infection • A long latent period without sign&symptom • Knee, hip, ankle • Fever may not be seen, a draining sinus can be observed
Mycobacterial Arthritis • Synovial fluid analysis: Leukocytes 10 000-20 000/ml, Acid-fast bacilli (AFB), culture………(80%) • Synovial biopsy; AFB, culture, histology (90%) • PCR • Anti-TB therapy (with 4 drugs) • Surgery; periarthricular abscess, reconstruction surgery
FUNGAL ARTHRITIS • Those with chronic disease/ immune suppression (Candida sp, Cryptococcus, Aspergillus), • In otherwise healthy people; direct trauma, penetrating trauma with foreign substance • In patients with immune suppression, trauma and hematogenous spread
Fungal Arthritis Treatment • Antifungal tx and surgery • Amphotericin B
Septicarthritis • Singlejoint (in most of thecases) • Knee, hip, shoulder,..