Download
1 / 40
510 likes | 1.33k Vues
Late Preterm Birth – What YOU Need to Know. Elizabeth McIntosh Chawla, MS4 Georgetown University School of Medicine 2009 Advocacy Project, Education of Resident Physicians on Late Preterm Birth, with the March of Dimes Maryland-National Capital Area Chapter.

E N D
Late Preterm Birth – What YOU Need to Know Elizabeth McIntosh Chawla, MS4 Georgetown University School of Medicine 2009 Advocacy Project, Education of Resident Physicians on Late Preterm Birth, with the March of Dimes Maryland-National Capital Area Chapter
Why are we talking about Preterm Birth? • Premature Birth Rates in the United States • One of the goals of US Healthy People 2010 is to REDUCE the preterm* birth rate in the US to 7.6% by 2010 • But rates have been INCREASING over the last decade • 9.1 % in 1981 • 11.6% in 1998 • 12.3% in 2003 • 12.7% in 2005 * Preterm Births refers to all infants born with <37 fully completed weeks. http://www.math.uni-luebeck.de/safir/Projects/Draeger/draeger.shtml
What about Late Preterm Birth? • Late Preterm Birth Rates • Of all preterm births, Late Preterm Births, 34 to 36 weeks, are both the largest and fastest growing subgroup • Since 1990, the rate of Very Preterm Birth (<32 weeks) has remained stable at 2% of live births • But between 1990 and 2003, Late Preterm Birth increased more than 20%, from 7.3% to 8.8% of live births, accounting for the majority of the increase in preterm birth rates over the last two decades1 • As of 2005, Late Preterm Births represent 9.1% of live births • Based on 2005 Data from the CDC on singleton births, Late Preterm Births made up about 72% of all preterm births2 1National Center for Health Statistics. 2003 final natality data. Data prepared by the March of Dimes Perinatal Data Center, 2005. 22008 NCHS Data Brief: Recent Trends in Infant Mortality in the US
Increase Most Striking in Late-Preterm Group 25% increase in Late Preterm Group Slide courtesy of Dr. Tonse Raju, 2007 presentation
2002 US DataPercent of Preterm Singleton Live Births (<37 wks) by Week of Gestation 36 wks 75% of singletonpreterm births 34wks 35 wks Source: NCHS, final natality data Prepared by March of Dimes Perinatal Data Center, April 2006. Slide courtesy of Dr. Tonse Raju, 2007 presentation
What about Washington, D.C.? • District of Columbia Preterm Birth Rates • In D.C., the rate of preterm births in 2005 was 15.9%,far above the national average of 12.7% 1 • The rate of Late Preterm Births was 10.4%, also far above the national average, which was 9.1% for this subgroup 1 • Disparities exist among population subgroups: • Race: preterm birth rates were highest for African Americans (18.2%) • Age: preterm birth rates were highest for women ages 40 and older (19.8%), followed by women under age 20 (17.6%) 1National Center for Health Statistics, final natality data. Data prepared by the March of Dimes Perinatal Data Center, 2005. www.marchofdimes.com/peristats
Disparities Among Races: National Statistics **The District of Columbia mirrors disparities seen across the United States: Preterm Births as a Percent of Live Births, by race and ethnicity, 1992 to 2003. SOURCE: CDC (2004a). Institute of Medicine, Report Brief: Preterm Birth: Causes, Consequences, and Prevention. July 2006
Why Should I Care? “Educating professionals includes enabling them to educate the public and patients. We need to begin by teaching what we now know with regard to preterm risks: maternal age, parity, prior preterm labor, multiple gestations, and behavioral (i.e., substance abuse/use, violence in patient’s life) and psychosocial factors. Professionals should understand why preterm birth is an important problem. All types of clinicians must be knowledgeable about core preterm birth issues because patient contacts with pediatricians, cardiologists, pharmacists, dental professionals, and others represent prevention and intervention opportunities. Health sciences curricula should be targeted to the discipline. The curricula for the clinicians and public health professionals responsible for primary and reproductive health care will need to be more comprehensive.” Statement from Report of the Surgeon General’s Conference on the Prevention of Preterm Birth, June 16-17, 2008
Why Should I Care? • Morbidity and Mortality is higherfor infants born between 34-36 weeks as compared to term infants.1 • In many cases, these complicationscan be prevented. • If you are a Pediatrician… • Infants born after 37 weeks have better overall outcomes. As physicians, it is your responsibility to advocate for your future patients, to give them the best chance at a healthy start and a healthy childhood. A few words of guidance to Mom at a well child visit can make a big difference! • If you are an OB/GYN… • The increase in rates of Late Preterm Births has been linked to rising rates of early induction of labor and c-sections. 1 For the health of your patient, and her unborn baby, keep in it there a little longer! • If you are a Family Physician… • For the health of both of your patients, Mom and baby, help them hang in there as long as possible. Full gestation is 40 weeks! • If you are a Medical Student… • Whether you are interested in perinatal outcomes or not, more knowledge makes you a better well-rounded physician, and more valuable to your patients. • And to everyone, knowledge is power, educate your patients on the facts! 1 National Center for Health Statistics. 2002 period linked birth/infant death data. Data prepared by the March of Dimes Perinatal Data Center, 2005.
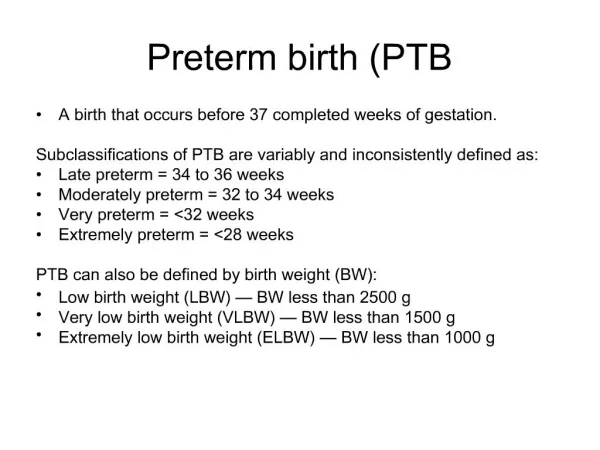
Late Preterm Birth: Some Definitions • Term – 370/7 to 416/7 weeks gestation • “Near Term” – terms such as near term, early term, moderate preterm, mild preterm, borderline preterm, etc. have been used in the past to describe infants born anywhere between 32-37 weeks • Late Preterm - NICHD [National Institute of Child Health and Human Development] Workshop 2005 recommended the use of “Late Preterm” to describe infants born between 340/7 to 366/7 weeks, or 239—259 days counting from the first day of the LMP. They also recommended discontinuing the use of the term “Near Term”. Late Preterm Infant Assessment Guide, Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN)
Gestational Age Terminology LatePreterm Firstdayof LMP 239 259 Day # 1 294 416/7 Week # 0/7 20 0/7 340/7 36 6/7 Preterm Term Postterm • Preterm: Prior to completion of 37th week (36 6/7 weeks; on or before 259th day) • Late Preterm: Between 34 0/7 through 36 6/7 weeks (239-259 days) * Raju TNK., Higgins RD, Stark AR, Leveno KJ Optimizing Care and Outcome of the Late Preterm (Near-Term) Pregnancy and the Late Preterm Newborn Infant. Pediatrics , 2006;118 1207-14 Drawingcourtesy: William Engle, MD, Indiana University * Slide courtesy of Dr. Tonse Raju, 2007 presentation
Why “Late Preterm” - not “Near Term”? • “Near-Term” conveys that these infants are almost term and therefore almost mature. • This may lead to false sense of security: less rigorous assessment in first hours of life, early discharge when infant is still at risk, inadequate follow-up plans. • “Late Preterm” conveys the sense that they stillpremature and still vulnerable . “All definitions are arbitrary, since maturation is a continuum” * Raju TNK., Higgins RD, Stark AR, Leveno KJ Optimizing Care and Outcome of the Late Preterm (Near-Term) Pregnancy and the Late Preterm Newborn Infant. Pediatrics , 2006;118 1207-14
What Causes Late Preterm Birth? • Medical Intervention: Early Induction of Labor and C-Sections • Incorrect assumption that 34-36 weeks is “close enough” given our current technological advances • Errors in dating of Gestational Age (women are poor historians), so “early” induction is accidental • Growing culture of the “patient as customer” – inductions and c-sections for non-medical reasons • Pre-term Labor: Spontaneous Premature Labor and PPROM • Can be due to maternal or fetal health complications • Increasing maternal age • Increases in multiples with modern fertility treatments
Late Preterm Cesarean Section and Labor Induction Rates among Singleton Live Births by Week of GestationUnited States, 1992 and 2002. 2002 C-S 1992 C-S 2002 Induction 1992 Induction Source: NCHS, final natality data Prepared by March of Dimes Perinatal Data Center, April 2006. Slide courtesy of Dr. Tonse Raju, 2007 presentation
Singleton Preterm Live Births: Reasons for Delivery from Birth Certificates 68% 57% 41% 29% 3% 2.2% Spontaneous Slide courtesy of Dr. Tonse Raju, 2007 presentation
Causes continued: Prevention • Medical Intervention: Early Induction of Labor and C-Sections • Correct dating of Gestational Age with early ultrasound – encourage prenatal care from the beginning of the pregnancy • Patient education about importance of continuing pregnancy until full term is reached – even if inconvenient to patient • Advocacy of OB/GYN residents to their colleagues – longer pregnancy has better maternal and fetal outcomes • Pre-term Labor: Spontaneous Premature Labor and PPROM • Smoking, alcohol, or drug use – cessation during pregnancy • Diabetes, hypertension – tight control, starting BEFORE conception • Infections – good prenatal care, treatment of active infection • Birth Defects – folic acid supplementation, proper immunization of Mom • Hx of preterm labor or preterm birth – good OB/GYN care, medical or surgical interventions if needed • Multiples – judicious use of assisted reproductive therapies (ART) • Social – decreasing stress, appropriate child spacing, avoiding extremes of maternal age, <20 years or >40 years Source: Report from the Surgeon General’s Conference on the Prevention of Preterm Birth, June 16-17, 2008
Later Neonatal Period Poor feeding and dehydration Readmission to hospital Early Infancy SIDS risk Later Outcomes Learning difficulties & School failures Behavior problems Medical Issues in Late-Preterm Infants • Transitional • Respiratory Distress (RDS) • Temperature Instability • Hypoglycemia • Feeding difficulties • First Week • Neonatal jaundice • Apnea • Infection rate 1 Late Preterm Birth: Every Week Matters, Medical Perspectives on Prematurity. Prepared by the Office of the Medical Director, March of Dimes. March 2006. 2Late Preterm Infant Assessment Guide, Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) 3 NICHD Workshop: Optimizing Care and Long-term Outcome of Near-term Pregnancy and Near-term Newborn Infant. July 18-19. Bethesda, MD, 2005.
Outcomes of Late Preterm Birth • The infant mortality rate among late preterm infants (7.7 per 1,000 live births) is three times higher than the rate among term infants (2.5 per 1,000 live births). [However, some of these higher rates are due to complications necessitating early delivery, including some birth defects, rather than due to early delivery itself.] • Late preterm infants incur greater costs and longer lengths of stay in neonatal intensive care units (NICU) and experience higher rates of re-hospitalization after neonatal discharge, as compared to term infants. • Children born in the late preterm phase have a greater risk of developmental delay, such as poor reading and math scores in elementary grades, need for special education, and retention in kindergarten than their full term counterparts. 1 Late Preterm Birth: Every Week Matters, Medical Perspectives on Prematurity. Prepared by the Office of the Medical Director, March of Dimes. March 2006. 2 2008 NCHS Data Brief: Recent Trends in Infant Mortality in the US 3 Chyi, L. et al. School Outcomes of Late Preterm Infants: Special Needs and Challenges for Infants Born at 32 to 36 Weeks Gestation. Journal of Pediatrics, July 2008.
School Outcomes of Late Preterm Infants Lisa J. Chyi, MD, Henry C. Lee, MD,MS, Susan R. Hintz, MD, MS, Jeffrey B. Gould, MD, MPH, and Trenna L. Sutcliffe, Md, MS Journal of Pediatrics, 2008
Methodology • Data Source • Publicly available ECLS-K dataset from the United States Department of Education [Early Childhood Longitudinal Study-Kindergarten Cohort] • Sample Group • Moderate Preterm: 32 to 33 weeks gestation (n=203) • Late Preterm: 34 to 36 weeks gestation (n=767) • Excluded children with any known complication at birth • Comparison group • Age equivalent classmates • Full Term: 37 to 41 weeks gestation (n=13,671)
Methodology contin… • Outcome Measures • 1) Reading and Math scores on Educational Tests (Including Peabody Tests and Woodcock Johnson Tests) • 2) Teachers Evaluation of the student’s Reading and Math abilities as compared to peers. Scored on a 5-point scale. (Most teachers unaware of students’ prematurity status) • 3) Presence of IEP or participation in Special Education Services, information provided by the schools • Evaluation • Outcomes were evaluated at K, 1st, 3rd, and 5th grade
Results: Distribution of Late Preterm Vs. Full Term across outcome categories Outcomes in Kindergarten * Values with P < .05
Results: Distribution of Late Preterm Vs. Full Term across outcome categories * Values with P < .05 Outcomes in 1st Grade
Results: Distribution of Late Preterm Vs. Full Term across outcome categories * Values with P < .05 Outcomes in 3rd Grade
Results: Distribution of Late Preterm Vs. Full Term across outcome categories * Values with P < .05 Outcomes in 5th Grade
Results Summary • Standardized Educational Tests • LP infants scored lower than FT infants for Reading in K and 1st grade, but not for Math • Teacher Evaluated Abilities as Compared to Peers • Reading: LP infants scored significantly lower in K, 1st , and 5th grades. • Math: LP infants significantly lower in K, 1st grade, with comparable math abilities in later grades • Special Education and IEPs • IEP: Greater % of LP infants required IEP in K and 1st grade, versus FT infants • Special Education: Greater % of LP infants in Special Education in K and 1st grade as compared to FT infants
Brain Development is a Continuum: At 34-35 weeks gestation, a baby’s brain is only 2/3 the size and maturity of full term.
As a Physician, What Can I Do? Healthy Moms make Healthy Babies, before, during, and after pregnancy! • Identify and Counsel patients (or Moms of your patients) on the preventable causes of Late Preterm Birth • Encourage Mom to plan ahead – the best prevention starts BEFORE conception: • Proper birth spacing improves perinatal outcomes • Get diabetes, hypertension, and other medical conditions under tight control BEFORE conception • Establish healthy weight, healthy diet, and supplementation with at least 400 mcg folic acid BEFORE conception • Talk to MD about immunizations and other preconception health recommendations BEFORE getting pregnant Reproductive Life Plan For more information about a Reproductive Life Plan and other counseling topics, please see www.physicianclassroom.org
As a Physician, What Can I Do? Healthy Moms make Healthy Babies, before, during, and after pregnancy! • Encourage Mom to see MD for good Prenatal care DURING pregnancy for best outcomes: • Correct gestational dating with early ultrasound • Help with managing infections or other health conditions that can put the infant at risk of complication • Start smoking cessation program, stop alcohol or drug use [or at least cut down as much as possible] during pregnancy • Learn the symptoms of preterm labor and seek help when necessary • Educate Mom about risks of late preterm birth, and what she can do for her part to ensure a full 40 weeks of gestation • Encourage good communication between Mom and healthcare providers AFTER birth to ensure good follow-up care for herself and the infant.
As a Physician, What Can I Do? • Understand and watch for specific medical complications in late preterm infants • Respiratory Distress • Hypoglycemia • Temperature instability/hypothermia • Feeding difficulties • Jaundice/hyperbilirubinemia • Keep a low threshold for NICU transfer • Prevent Re-hospitalization • Thoroughly evaluate infant before sending home • Anticipate possible complications • Arrange for appropriate follow-up • Appropriately Educate Parents of Late preterm Infants on special health considerations and what to watch for
Educating Parents: What to Watch For in Your Late Preterm Infant Segment of Patient handout found at www.awhonn.org
More Examples of Patient Handouts: DRAFT This and other patient handouts available through your local March of Dimes office.
Conclusion “There are misconceptions outside of the OB/GYN community that preterm birth (especially late preterm) is not a major problem; therefore, content on preterm birth risks and the consequences of preterm birth needs to be included in the curricula of all medical specialties, as well as in training for allied health and public health professionals.” [Statement from Report of the Surgeon General’s Conference on the Prevention of Preterm Birth, June 16-17, 2008]
Conclusion Knowledge is Power Educate yourselves Educate your colleagues Educate your patients Together we can make a big impact on the number of late preterm infants born in the United States with just a little knowledge and prevention…
Acknowledgements • March of Dimes Foundation • Dona Dei, RN, MSN • Dr. Tonse N. K. Raju, MD, DCH • Dr. Matthew Levy, MD, MPH
References • National Center for Health Statistics. 2002-2005 final natality data. Data prepared by the March of Dimes Perinatal Data Center, 2005. • 2008 NCHS Data Brief: Recent Trends in Infant Mortality in the US. • Institute of Medicine, Report Brief: Preterm Birth: Causes, Consequences, and Prevention. July 2006. • Report from the Surgeon General’s Conference on the Prevention of Preterm Birth, June 16-17, 2008. • Late Preterm Infant Assessment Guide, Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) • Late Preterm Birth: Every Week Matters, Medical Perspectives on Prematurity. Prepared by the Office of the Medical Director, March of Dimes. March 2006.
References contin… • Raju TNK., Higgins RD, Stark AR, Leveno KJ Optimizing Care and Outcome of the Late Preterm (Near-Term) Pregnancy and the Late Preterm Newborn Infant. Pediatrics , 2006;118 1207-14 • Chyi, L. et al. School Outcomes of Late Preterm Infants: Special Needs and Challenges for Infants Born at 32 to 36 Weeks Gestation. Journal of Pediatrics, July 2008 • Raju TN. Epidemiology of late preterm (near-term) births. [Review] [53 refs] Clinics in Perinatology. 33(4):751-63; 2006 Dec. • Jain S. Cheng J. Emergency department visits and rehospitalizations in late preterm infants. [Review] [16 refs] Clinics in Perinatology. 33(4):935-45; 2006 Dec. • Adamkin DH. Feeding problems in the late preterm infant. [Review] Clinics in Perinatology. 33(4):831-7; 2006 Dec. • Fuchs K. Wapner R. Elective cesarean section and induction and their impact on late preterm births. Clinics in Perinatology. 33(4):793-801; 2006 Dec.
References contin… • Websites • www.marchofdimes.com • www.awhonn.org • www.marchofdimes.com/peristats • www.iom.edu • www.surgeongeneral.gov • www.cdc.gov/nchs