Traditional Hernia Repair
380 likes | 1.61k Vues
Traditional Hernia Repair. Basic Format Herniorrhapy. Objectives. Assess the anatomy, physiology, and pathophysiology of the abdomenal wall. Analyze the diagnostic and surgical interventions for a patient undergoing a herniorrhapy.

Traditional Hernia Repair
E N D
Presentation Transcript
Traditional Hernia Repair Basic Format Herniorrhapy
Objectives • Assess the anatomy, physiology, and pathophysiology of the abdomenal wall. • Analyze the diagnostic and surgical interventions for a patient undergoing a herniorrhapy. • Plan the intraoperative course for a patient undergoing inguinal herniorrhapy. • Assemble supplies, equipment, and instrumentation needed for the procedure.
Objectives • Choose the appropriate patient position • Identify the incision used for the procedure • Analyze the procedural steps for inguinal herniorrhaphy. • Describe the care of the specimen • Discuss the postoperative considerations for a patient undergoing pt w/inguinal herniorrhaphy.
Terms and Definitions • Hernioplasty or herniorrhaphy • Hesselbach’s Triangle • Transversalis fascia • Reducible hernia • Incarcerated hernia • Strangulated hernia
Definition/Purpose of Procedure • Definition • A sac lined by peritoneum that protrudes thru a defect n the layers of the abdominal wall; congenital, acquired, traumatic; generally covered by tissues, a peritoneal sac, and any contained viscera • Purpose • To repair the defect and strengthen the supporting structures
Relevant A & P: Tissue Layers • (STST p. 404 descending order) • Skin and subcutaneous • Scarpa’s fascia • Innominate fascia • Interparietal fascia • Internal oblique muscle • Transverse abdominal muscle • Transverse fascia • Cooper’s ligament • Rectus Abdominis muscle • Peritoneum
Relevant A & P: Other structures • Superficial & inferior epigastric muscles • Iliofemoral vessels • Spermatic cord and blood supply • Ilioinguinal nerve • Lacunar ligament • Inguinal ligament (Poupart) • Conjoined ligament (Falx inguinalis) • Cremaster muscle & fascia • Hesselbach’s Triangle • Femoral canal • Iliopubic tract
Pathophysiology • Protrusion of an organ or part of an organ through a defect in the supporting structures which normally contain it • Transverse fascia is the man focus of groin herniation and separates the abdominal musculature from the preperitoneal fat. It is a continuation of the fascia completely containing the abdominal cavity and is inherently weak in the area of Cooper’s Ligament and the iliopubic tract, lending to inguinal herniation.
What is a Direct Hernia? • Direct • Acquired weaknesses in transversalis fascia • Location: Hesselbach’s triangle • Causes • Emerge between the deep epigastric artery and rectus abdominus muscle and protrude into the inguinal canal but not into the spermatic cord • More difficult to repair • Men
What is an Indirect Hernia? • Congenital or acquired weaknesses in transversalis fascia • Location: lateral to deep epigastric vessels • Protrude through inguinal ring and pass with the spermatic cord structures down the inguinal canal; may descend into the scrotum • Men
Diagnostics • Exams: asked to stand and cough during physical exam: can see outpouched area; fingertip palpation –can feel edges of external ring and or abd wall. Pt most likely will have pain; may be described as burning. Compare both sides for protrusions. • Preoperative Testing: Routine CBC, ECG or chest as applicable; can employ CT, herniography, & std radiography if dx not confirmed
Surgical Intervention:Special Considerations • Patient Factors • Possibly in pain • Room Set-up : Routine
Surgical Intervention: Anesthesia • Method: Various: General, Spinal, Epidural, Regional w/sedation, Local • *Surgeon may ask for pt to cooperate by coughing or bearing down • Equipment
Surgical Intervention: Positioning • Position during procedure • Supine w/arm boards • Supplies and equipment • Special considerations: high risk areas
Surgical Intervention: Skin Prep • Method of hair removal—at least on side of hernia down to groin—ask • Anatomic perimeters—table side to table side; upper abdomen to mid thigh • Solution options—Routine (Betadine vs Hibclens)
Surgical Intervention: Draping/Incision • Types of drapes: Lap Sheet • Order of draping: 4 towels & sheet • Special considerations • State/Describe incision: Anterior Groin/oblique inguinal incision
Surgical Intervention: Supplies • General • Lap pack, gowns, raytex, disposamag • Specific • Suture: Various (Mayo and Ferguson taper type needles) • After the hernia repair, finer sutures will be used for other layers of tissue • Examples: 3-0 silk ties, 2-0 silk SH (GI), 3-0 silk, 0 silk (GI needle); 3-0 vicryl ; Other possible: 2-0 Prolene SH, 0 Ethibond, 4-0 Vicryl undyed • For mesh: 0 Prolene CT-1 or CT-2 • Kittners • Blades: # 10 x 2 • 35 R stapler (hold)
Surgical Intervention: Supplies cont’d • Medications on field (name & purpose) • For local: Example: Xylocaine .5% w/Marcaine .25% w/epi • 20 cc syringe, 25 g needle, possibly 22 g spinal needle • Catheters & Drains: A ½ in penrose drain is used to retract spermatic cord structures
Surgical Intervention: Instruments • General • Minor set • Specific • A hemostat is placed on the penrose drain before passing to the surgeon • Med debakeys • Med rt angles • Gelpies x 2
Surgical Intervention: Equipment • General: Standard • Specific
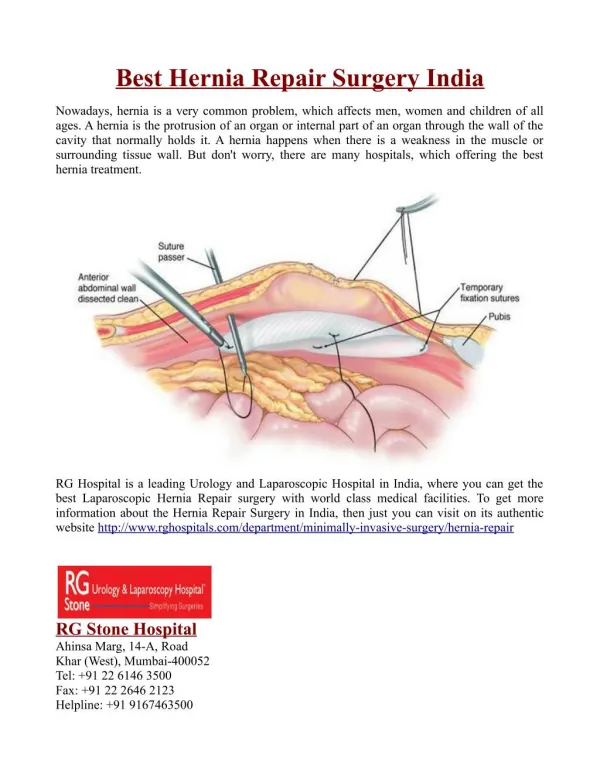
Procedure Highlights • 1. Layers of the abdominal wall are incised • 2. The spermatic cord is identified & dissected free • 3. The hernia sac is identified • 4. The sac is ligated and removed. • 5. Layers of the wound are closed individually.
Surgical Intervention: Procedure Steps • After prep, pt is draped with groin area exposed on affected side • Incision is made over hernia site and electrocautery used for hemostasis • Surgeon incises fascia lying over the spermatic cord and retracts w/several hemostats on the edge of the incised fascia • Surgeon identifies spermatic cord and separates it from the surrounding tissue • STSR mounts moistened Penrose drain on a med clamp & passes it to the surgeon, who passes it around the spermatic cord for retraction
Surgical Intervention: Procedure Steps Cont’d • Dissection continues until hernia is located • Hernia repair • Direct • Surgeon sutures transversalis fascial defect using heavy interrupted sutures as STSR initiates first closing count • Surgeon closes external oblique fascia as SRST initiates second closing count
Surgical Intervention: Procedure Steps Cont’d • Hernia repair • Indirect • Surgeon dissects sac away from the spermatic cord using Metzenbaum scissors • The sac is opened & edges grasped with hemostats • Surgeon pushes contents of sac back toward the abdomen w/ a finger or a small sponge on instrument
Surgical Intervention: Procedure Steps Cont’d • Surgeon ligates small sac, uses purse-string suture, or oversews to close large sac as STSR initiates first closing count • Surgeon sutures transversalis fascial defect using heavy (0, 2-0) interrupted sutures as STSR initiates second closing count.
Classic Procedures • Marcy repair • Closure of inguinal ring • Bassini or Bassini-Shouldice Repair • A new inguinal canal is made by uniting the edge of the internal oblique muscle to the inguinal ligament • McVay/Lotheissen • The transverse abdominis muscle & its associated fasciae (transverse layer) are sutured to the pectineal ligament (Cooper’s ligament repair)
Summary for Hernias • Dissection: Identify the structures • Repair : Reduce the hernia; Repair the defect • Closure
Counts • Initial • First closing • Final closing • Sponges • Sharps • Instruments The peritoneal cavity may be entered when the hernia sac is opened—Counts must be done!
Dressing • Types & sizes • 2x2 or 4x4, ½ in steri strips, Small Tegaderm • Type of tape or method of securing • May use Mastisol or Benzoin
Specimen & Care • Identified as Peritoneal hernia sac (Indirect) • Handled: Routine in formalin fixative
Postoperative Care • Destination • PACU • Expected prognosis (Good)
Postoperative Care • Potential complications • Hemorrhage • Infection • Other: Damage to…neural and vascular structures • Recurrence • Ischemic orchitis & testicular atrophy • Loss of bowel function • Surgical wound classification: 1
Resources • Alexanders: pp. 433-439 • Berry & Kohn pp. 668 • Lemone and Burke Ch 24, pp. 677-679 • MAVCC Unit 3 pp. 45-81 • STST Ch 14 pp. 405-407