Download

1 / 45
450 likes | 453 Vues
International Quality Improvement Collaborative for Congenital Heart Surgery. Vision. Facilitate a collaborative of healthcare teams from around the world creating a culture of patient safety & quality for children receiving congenital heart surgery in developing countries. Mission.

E N D
International Quality Improvement Collaborative for Congenital Heart Surgery
Vision Facilitate a collaborative of healthcare teams from around the world creating a culture of patient safety & quality for children receiving congenital heart surgery in developing countries
Mission Our mission is to reduce mortality and major complications for children undergoing congenital heart surgery.
Objective • Create tailored quality improvement strategies to reduce mortality and major complications for developing world programs. • Employ a telemedicine platform to facilitate distance learning, dialogue, disseminate knowledge & skills.
Drivers of Mortality • Team-based practice through nurse empowerment • Reduce surgical site infections and bacterial sepsis • Safe perioperative practices
Change Strategies Key Drivers Aim Utilize a surgical safety checklist to prompt and document evidence-based process measures (i.e. antibiotics given within 60 minutes of surgical incision) Safe Operative Practice Focus on hand hygiene for ALL clinical personnel in contact with patient care. Reduction In 30 day mortality associated with congenital heart surgery Reduce Surgical SiteInfections & Bacterial Sepsis Empowering nurses Evidence-based nursing practice Scripting nurses in ward and ICU on how to give reports Accurate 24hr total patient intakes and outputs Accurate daily recording of patient weight Effective Communication-SBAR Team-based Practice Key Driver Diagram
Learning Modules • Learning Module I: Team-based practice and nurse empowerment • Learning Module II: Reducing surgical site infection and bacterial sepsis • Learning Module III: Safe perioperative practice
Learning Modules • Contain quality improvement strategies for each of the 3 drivers that impact mortality addressed during the webinars. • Each module contains a series of 3 educational sessions. • Sessions advance from beginning, intermediate, and advance-level of learning & acquisition of skills.
Timeline for Webcasts The color of each Learning Module corresponds to the date the that topic will be presented during that month’s webcast. For example, Team-based Practice will be the topic 2/17, 5/19, and 8/18.
Data Entry Map Founding Sites New Sites No Data Entry
Cumulative Site Participation *Graph captures only sites that have entered > 10 patients into the IQIC Database.
Safe Perioperative Practice Learning Module Implementation of a surgical safety checklist for congenital cardiac surgery (Session I)April 21, 2010
Outline • Surgical safety as a global public health concern • Why use a checklist to improve surgical safety? • The landmark World Health Organization (WHO) surgical checklist study • Development of a checklist for congenital heart surgery • Strategies to successfully implement the checklist
Surgical Safety: A Global Public Health Concern Approximately 234 million operations are performed globally each year 1 million deaths and 7 million disabling complications occur each year worldwide Surgical complications are common and often preventable
Why use a team-based surgical safety checklist? • Facilitates compliance with evidence-based standards of care (process measures) • Enhances communication and team dynamics during complex procedures • Establishes (and reinforces) the importance of a “safety” culture within the operative environment
WHO Surgical Safety Checklist • Collaborative effort between surgeons, operating room nurses, anesthesiologists, and human behavior experts • Developed a standardized framework based on evidence-based practices for safe surgical and anesthetic care
WHO Surgical Safety Checklist:“Sign-In” section Performed by the circulating nurse togetherwith the anesthesiologist: Verifies correct patient, procedure(s) and operative site Reviews potential anesthesia-related complications (airway emergencies) Ensures adequate intravenous access for expected blood loss
WHO Surgical Safety Checklist:“Time-out” portion Performed by the ENTIRE TEAM: Begins with introductions of all team members Final review of correct patient, procedure & site Surgeon reviews case elements which may impact management by other team members Anesthesia reviews the adequacy of airway and intravenous access based on the surgeon’s comments Nursing reviews availability and satisfactory function of equipment needed for case
WHO Surgical Safety Checklist:“Sign-Out” portion Performed by the ENTIRE TEAM: Verification of procedure performed and sponge and instrument counts Review of equipment and plan to address defective or malfunctioning equipment if indentified Review of concerns during the immediate post-operative period (airway, bleeding, monitoring)
The Checklist was piloted in 8 cities… EURO EMRO PAHO I London, UK Amman, Jordan Toronto, Canada WPRO I Manila, Philippines PAHO II Seattle, USA WPRO II Auckland, NZ AFRO Ifakara, Tanzania SEARO New Delhi, India
Study Design • Pre and post-interventional study following implementation of the WHO safe surgery checklist • 4,000 patients targeted between all centers for each of the pre and post-intervention groups • Outcome measures: - 30-day mortality rate - 30-day major complication rate (all-cause) - Compliance with peri-operative process measures
WHO Study:Outcome Measures Complications: Intubation > 48 hours Graft/implant failure Urinary tract infection Stroke Surgical site infection Blood transfusion Cardiac arrest Deep venous thrombosis Pulmonary Embolism Unplanned re-intubation Sepsis Acute renal failure Wound dehiscence Peripheral nerve injury Coma > 24 hours Unplanned re-operation Process measures: Adequate IV access for blood loss Appropriate use of pulse oximetry Objective preop airway evaluation Verification of patient and procedure Verification of sponge/instrument count Antibiotics given within 1 hour of incision
Results of the WHO study • Operative mortality reduced by 47% • 30-day morbidity reduced by 36% • Compliance with evidence-based process measures increased from 34 to 57% • Reduction in morbidity and mortality occurred even in the absence of improved compliance with process measures
Survey of Attitudes to Checklist Use Among Clinicians at Study Sites (n=229)
Development of a checklist designed for congenital heart surgery • WHO checklist used as a conceptual framework • Modified for congenital cardiac surgical procedures • Increased emphasis on team dynamics • Emphasis on specific roles for each team member • Increased focus on the transfer of care from the operating room to the critical care environment (safe hand-off)
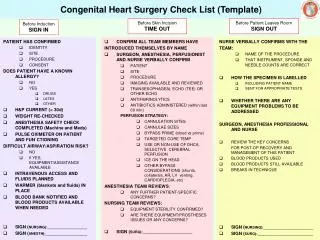
Congenital Heart Surgery Check List Before Induction SIGN IN Before Skin Incision TIME OUT Before Patient Leaves OR SIGN OUT HAVE THE SURGEON AND CIRCULATOR TOGETHER CONFIRMED: • SURGICAL PROCEDURE(S) PERFORMED? • INSTRUMENT, SPONGE, AND NEEDLE COUNTS? HAVE THE CIRCULATOR AND ANESTHESIOLOGIST TOGETHER CONFIRMED: • PATIENT IDENTITY? • OPERATIVE SITE(S)? • PROCEDURE(S) TO BE PERFORMED? • MEDICATION ALLERGIES? • PLAN FOR KEEPING PATIENT WARM? • NEED FOR BLOOD PRODUCTS • IF YES, HAS THE BLOOD BANK BEEN NOTIFIED? HAS THE ANESTHESIOLOGIST CONFIRMED: • IV ACCESS IS ADEQUATE FOR ANTICIPATED PROCEDURE(S)? • POSSIBILITY OF DIFFICULT AIRWAY/ASPIRATION? • IF YES, HAS A PLAN BEEN DISCUSSED TO ADDRESS THIS POSSIBILITY? • HAVE ALL TEAM MEMBERS INTRODUCED THEMSELVES BY NAME AND ROLE? HAS THE SURGEON VERBALLY CONFIRMED TO TEAM: • CORRECT PATIENT, SITE, AND PROCEDURE(S)? • RELEVANT IMAGING AND STUDIES REVIEWED? • EQUIPMENT SETTINGS APPROPRIATE? • ANTICIPATED LENGTH OF PROCEDURE(S)? • NEED FOR IMPLANTS OR OTHER PROSTHETICS? HAS THE PERFUSIONIST VERBALLY CONFIRMED: • RELEVANT DETAILS REGARDING CANNULAE? • TARGETED CORE TEMPERATURE? • NEED FOR SELECTIVE CEREBRAL PERFUSION AND/OR CEREBRAL COOLING WITH ICE? • NEED FOR CIRCULATORY ARREST, SHUNTS, COLLATERALS, AR, LV VENTING, OR CARDIOPLEGIA? HAS THE ANESTHESIOLOGIST VERBALLY CONFIRMED: • ANTIBIOTICS GIVEN WITHIN 60 MINUTES OF INCISION? • PLAN FOR REDOSING ANTIBIOTICS DURING CASE? HAS THE CIRCULATING NURSE VERBALLY CONFIRMED: • CONSENT MATCHES PROCEDURE(S) VERBALIZED ABOVE? • AVAILABILITY OF IMPLANTS/PROSTHETICS (IF NEEDED)? EACH TEAM MEMBER MUST VERBALIZE THEY HAVE NO CONCERNS WITH PROCEEDING SAFE HANDOVER TO ICU HAS THE SURGEON DISCUSSED: • THE NATURE OF THE REPAIR/PROCEDURE(S)? • COMPLICATIONS & RISK FOR FURTHER BLEEDING? HAS THE ANESTHESIOLOGIST DISCUSSED: • CONCERNS REGARDING AIRWAY MANAGEMENT? • HEMODYNAMIC STABILITY AND PRESSOR SUPPORT? • PLAN FOR VENTILATION MANAGEMENT? • TEE FINDINGS & SATURATION DATA DURING CASE? • AVAILABILITY OF BLOOD PRODUCTS IF NEEDED? • HAS THE ANESTHESIOLOGIST, SURGEON AND ACCEPTING CRITICAL CARE PHYSICIAN DISCUSSED THE NEED FOR LABS/IMAGING OVER THE NEXT 24 HOURS?
Implementing the Checklist:Strategies for Successful Pilot • Identify leaders from each discipline • Promote the checklist at your institution • Begin by piloting on a small scale • Obtain feedback from all team members • Gradual expansion to multiple operating rooms/teams
Identify checklist leaders from each discipline for the pilot phase • Identify the checklist “triad”: surgeon, operating room nurse & anesthesiologist • “Triad” members ideally should be senior & influential among their peers • Leaders will eventually play role in changing the safety culture through education and auditing
Using the checklist effectively inside the operating room • Checklist should be visible to all team members at the same time – laminated wall posters work well
Using the checklist effectively inside the operating room • Sterile checklists can be used as a reminder to direct attention to the wall-mounted checklist • Operating room circulator should document compliance with the checklist for later review
Strategies to promote the checklist at your institution • Email and newsletters announcing the checklist • Web-based education and teaching-rounds for all relevant operating room personnel • PowerPoint presentations to illustrate the potential of using checklists to improve safety
Obtain feedback from all team members • What went well? • What could have gone better? • How should the checklist protocol be modified to fit the needs of your institution? • Keep a detailed log of feedback comments
Next Steps: From piloting to widespread implementation Our team will have periodic conference calls with you to review feedback and troubleshoot implementation challenges Engage in an on-going process of modifying the checklist to meet the needs of your institution Develop strategies for auditing and training as the checklist is adopted into broad practice
Resources Resources Provided WHO Surgical Safety Checklist WHO Guidelines for Safe Surgery WHO Starter Kit and WHO Implementation Manual Additional resources available online www.who.int/safesurgery www.safesurg.org