Download

1 / 31

E N D
1. Improving Care for Diabetic Patients
Jim Mold, M.D., M.P.H.
The University of Oklahoma
Department of Family and Preventive Medicine
3. Research Question
Why don�t physicians always achieve a perfect score on diabetes quality of care audits?
4. Methods: Approximately 2000-2001
All diabetic patients >50 years of age followed by participating OKPRN physicians for at least one year and seen by them within the last 3 months
OFMQ chart audit to determine if DQIP targets were met
5. Methods A1c in past year
Lipid panel in past 2 years
UA for protein in past year
Eye exam in past year
Foot exam in past year
ACEI for HTN and/or proteinuria
Flu shot in past year
Pneumococcal vaccine ever
6. Methods Audit report left on each chart with a survey instrument requesting physician to indicate reasons for not meeting each of the unmet targets
Eight fixed choices plus �other�
7. Results Audits are not perfect
Auditors counted off for no microalbumin when UA showed protein or patient already on an ACEI
Auditors counted off if had flu shot early last year and late this year (>1 year)
Different reasons for different quality indicators
8. Results/Reasons A1c: not indicated
UA, micro-albumin: forgot or not indicated
Retinal exams and foot exams: done but report/findings not in chart (documentation problem)
9. Results/Reasons Flu shot: offered/declined (documentation problem)
Pneumovax: as for flu; �inadequate reimbursement�
BP<130/80, A1c<9.5, LDL<130: pt. making progress; non-adherence
10. Summary
Optimal audit scores are less than 100% (probably 85-90% depending upon patient population)
Improvement will probably require several different interventions (a flow sheet is not likely to improve all indicators)
11. Project #2 BP Control in Diabetic Patients
Adam Cotton, MS2
Jim Mold, MD, MPH
Cheryl Aspy, PhD
12. Research Question
Why do PCP�s sometimes not attempt to lower BP below 130/80 in their diabetic patients?
Assumption: There are a variety of legitimate clinical reasons for not doing so.
13. Methods Consecutive diabetic patients seen by eight participating OKPRN physicians
Clinic note reviewed by a medical student
If BP>130/80 AND physician�s note did not mention any change in strategy, student interviewed physician (within 2 weeks of the index visit)
Structured interview
Audiotaped and transcribed
14. Methods Transcribed interviews reviewed separately by the three investigators
Coded for categories of reasons
Categories reviewed by group and differences resolved
15. Results Clinician Factors
Patient Factors
Information/Measurement Factors
16. Clinician Factors Co-management (e.g. BP co-managed by another physician)
Competing demands (e.g. patient presented with acute problem)
Satisfied with progress/waiting for full effect of medicine
Should generally take 6 weeks max.
Disagreement with ADA guidelines
Only 1 of 9 physicians
17. Patient Factors Limited options (e.g. financial constraints, multiple other meds, ESRF)
Adherence problems (e.g. cognitive deficits, mental health problem, language/cultural barrier, denial)
Competing agendas (e.g. different goals than clinician)
Unfavorable risk:benefit ratio
18. Information/Measurement Factors Documentation error (BP or intervention not recorded)
Insufficient or confusing information
Patient missed dose of meds
Lack of consistent trend
Explanation/rationalization (pain, stress, exertion)
Home readings normal/office readings high
19. Conclusions Many reasons for not lowering BP to target
Physician factors, patient factors, measurement factors
Measurement factors might be ameliorated by 24 BP monitoring
20. Project #3 Improving Diabetes Care Using Best Practices Research and Practice Enhancement Assistants
Jim Mold, MD, MPH
Margaret Enright, MPH, CDE
W. H. Oehlert, M.D.
Dale Bratzler, D.O.
K.D. Walkingstick, MS
21. Research Question Can the quality of diabetes care be improved by a three part intervention:
Feedback on performance with benchmarking
Instruction of clinicians in principles derived from exemplar interviews
Practice enhancement assistants to facilitate practice changes
Compared to clinician feedback/benchmarking alone?
22. Methods Pre- and post-intervention change with historical comparison group that received feedback with benchmarking
All audits performed by trained OFMQ auditors
Duration of Study: 9 months
1 month to identify the �best practice� principles
4 months of pre-intervention data (June-Aug)
4 months of post-intervention data (Oct-Jan)
23. Outcome Measures
DQIP Indicators (same as for study #1)
We also collected data on mammography (within 2 years) as a control variable
24. Methods (cont.) From existing audit data, OFMQ staff identified 5 OKPRN clinicians with exemplary performance
90% of records met two or more of diabetes care indicators
Two or more exemplars for each diabetes care indicators
25. Methods (cont.) Exemplars interviewed by OFMQ nurse by phone
Interviews transcribed
From transcripts, three researchers identified and agreed upon a set of 6 principles of exemplary care
Mold JW and Gregory ME Best practices research. Family Medicine 2003, 35 (2): 131-134
26. Methods (cont.) Dr. Mold visited each physician and presented the six principles
and
The project provided them with a practice enhancement assistant (PEA) to assist with implementation
In the practice approximately 1/2 day every week for 4 months
They were also provided with feedback from the pre-intervention audits
27. Methods (cont.) We also made available a PDA Diabetic Patient Tracking application conceived of by an OKPRN physician and developed by us prior to this project
Prompts the nurse (or physician) to follow guidelines
Creates an auditable registry of diabetic patients
Produces a flow sheet for the medical record
28. Principles Derived from Exemplar Interviews Diabetes visits EVERY 3 months for every diabetic patient
Label diabetic charts with sticker
Protocol for office staff (triggered by sticker)
Keep a registry of all diabetic patients
Work with one or two eye doctors who are faithful about sending reports and recalling patients
Flow sheet for chart
29. Results (Process Measures) High rate of acceptance of six principles
Mean of 4/6 principles implemented
High acceptance of the PDA-based diabetic registry
21/30 decided to to use it
30. Results (Outcome Measures) All diabetic patients > 50 y.o. seen during that 3 month period (pre- or post-intervention) and followed for at least 1 year
25 physicians
595 pre-intervention patients
582 post-intervention patients
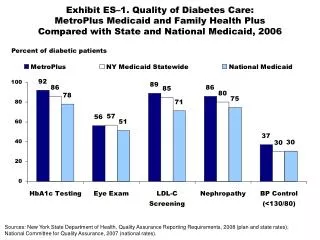
31. Quality of Care Indicators A1c: 87% ? 96% p=0.0003
UA protein: 53% ? 64% p=0.05
Lipid Panel: 69% ? 80% p=0.02
Foot Exam: 71% ? 82% p=0.004
Retinal Exam: 48% ? 59% p=0.04
Pneumovax: 42% ? 61% p=0.0006
ACEI for BP: 72% ? 86% p=0.03
ACEI for prot: 53% ? 64% p=0.05
Paired t-tests; physician as unit of analysis
32. Comparison Groups Mammography rates unaffected by the intervention
OFMQ benchmarking study (feedback plus a reasonable performance target based upon 90th percentile of peer performance) showed no significant improvements in DQIP indicators in a similar group of practices the previous year
33. Conclusions Significant short-term improvement in physician performance with instruction in principles derived from exemplars plus assistance of a PEA
High level of physician acceptance of the exemplar principles and the PEA
34. Limitations Historical control
Others have reported benefit of benchmarking
Short term follow-up
Can�t separate individual components of the intervention
Exemplar principles
PEA
PDA application
35. Project #4 RCT to Determine Relative Effectiveness of Feedback/Benchmarking, Best Practice Principles, and PEAs
Three arms with 8 practices in each arm
Audit/feedback/benchmarking (FB)
FB + Best Practice Principles (BPP)
FB + BPP + Practice Enhancement Assistant (PEA)
36. Methods FB FB+BPP FB+BPP+PEA
Clinics 8 8 8
Clinicians
Pre- 14 14 10
Post- 11 14 10
Patients
Pre- 474 332 387
Post- 481 372 315
37. Results A1c in 1 yr (mean A1c)
Pre- Post-
FB 71% (7.4) 94% (6.7)
FB/BPP 87% (7.9) 85% (7.4)
FB/BPP/PEA 75% (7.2) 83% (7.1)
38. Results Lipids in 1 yr (mean LDL)
Pre- Post-
FB 54% (111) 81% (102)
FB/BPP 64% (114) 70% (110)
FB/BPP/PEA 66% (104) 71% (106)
39. Results Foot exam/1 yr (eye exam/1 yr.)
Pre- Post-
FB 59%(35%) 63%(56%)
FB/BPP 74% (55%) 61% (59%)
FB/BPP/PEA 62% (41%) 39% (44%)
40. Results Taking an ACEI
Pre- Post-
FB 57% 66%
FB/BPP 65% 67%
FB/BPP/PEA 61% 51%
41. Results Pneumovax ever
Pre- Post-
FB 20% 46%
FB/BPP 56% 54%
FB/BPP/PEA 39% 42%
42. Results Degree of practice implementation (degree of personal implementation) 1�10 scale
FB 8.2 (8.6)
FB/BPP 5.2 (5.9)
FB/BPP/PEA 7.4 (7.1)
43. Results Difficulty for practice with implementation (personal difficulty) 1-10 scale
FB 5.2 (4.3)
FB/BPP 6.5 (5.7)
FB/BPP/PEA 4.3 (3.9)
44. Results Satisfaction with practice�s management of diabetics (your management) 1-10 scale
Pre- Post-
FB 6 (6.4) 8 (8.2)
FB/BPP 5 (6.1) 6.5 (7.2)
FB/BPP/PEA 5.4 (5.5) 7.9 (8)
45. Conclusions There was some improvement in performance overall in all groups
Audit/feedback/benchmarking alone may have worked as well or better than with addition of best practice principles and a PEA
Why????
46. Speculations Small numbers/randomization failure
Different levels of motivation/readiness to change
Different levels of ability to change/control over processes
FB Group paid more attention to their audit results and knew they were going to have to address them without help
PEAs used ineffective techniques
47. Questions/Reference