Download
1 / 47
480 likes | 822 Vues
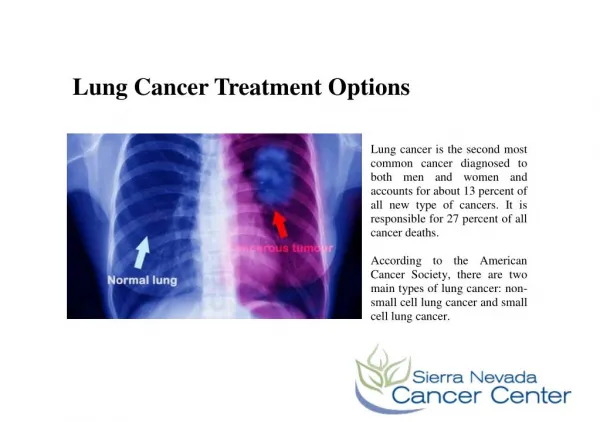
Treatment Options. Chapter 10 Olive Peart MS, RT (R)(M) www.opeart.com. BREAST CANCER TREATMENT. Breast cancer is not an emergency Second opinions are often recommended Treatment options include surgery, radiation, drugs—or any combination

E N D
Treatment Options Chapter 10 Olive Peart MS, RT (R)(M) www.opeart.com
BREAST CANCER TREATMENT • Breast cancer is not an emergency • Second opinions are often recommended • Treatment options include surgery, radiation, drugs—or any combination • Treatment cannot begin until stage, size, and location of cancer is known
STAGING BREAST CANCER • Stage grouping classifies breast cancer patients in 4 stages (Stages 0-IV). • A patient’s stage depends on the extent of the primary tumor, the spread of the cancer to regional lymph nodes, and whether there is distant metastasis. • In staging, lower numbers represent less spread of the cancer. • The tumor, represented by the letter ‘T,’ describes size of the cancer. • The lymph node involvement, represented by ‘N,’ indicates the number of nodes involved. • Men with breast cancer can be treated with the same criteria. • Tumor margins, tumor size, and the number of positive axillary nodes are just as important in planning treatment for male breast cancer patients as in female patients
TUMOR MARKERS • Breast tumors are currently classified using five immunohistochemical (IHC) tumor markers: • Estrogen receptor (ER+) • Progesterone receptor (PR+) • Human epidermal growth factor receptor 2 (ERBB2, formerly HER2 or HER2/neu) • ERBB1(HER-1) • Cytokeratin 5/6 (CK 5/6) • About 2 out of 3 breast cancers have at least either the ER+ or the PR+ receptors. • Cancers with the HER2/neu protein marker do not respond to treatment with tamoxifen or other antiestrogen drugs. • Normally, HER2 receptors help control how a healthy breast cell grows, divides, and repairs itself. The HER2/neu gene instructs the cells to make this protein.
MASTECTOMY • Mastectomy • Surgical removal of the entire breast • Radical mastectomy • Entire breast plus lymph nodes, chest wall, and muscle • Modified radical mastectomy • Entire breast plus lymph nodes • Skin-Sparing Mastectomy (SSM) • Resection of the nipple and areola complex, removal of any existing surgical or biopsy scar • Quadrantectomy or partial mastectomy • Removes a quarter of the breast, including the tumor
COMPLICATIONS OF MASTECTOMY • Wound infection • Hematoma • Seroma • Lymphedema • Numbness in upper arm and skin • Phantom breast pain
LUMPECTOMY • Removal of the breast cancer tumor and the surrounding margins of the normal breast tissue.
POOR CANDIDATES FOR LUMPECTOMY • Multiple cancers in one or both breast • Prior radiation to chest/breast area • Previous lumpectomy • Connective tissue disease, e.g., rheumatoid arthritis, osteoarthritis • Pregnancy • Large tumors in small breast • Larger tumors
LYMPH NODE BIOPSY • To determine cancer spread to the lymph nodes • Required axillary node dissection • Removal of the underarm lymph nodes • Needs general anesthesia • Often performed at the time of lumpectomy or mastectomy • Complication include lymphedema Alternative option include • Sentinel lymph node biopsy • Removal of the 1 first node in the lymphatic chain plus 2-3 others
COMBINATION THERAPY • Lumpectomy is often combined with • Radiation therapy • and/or chemotherapy • and/or Tamoxifen
COMPARISONS OF SURGICAL TREATMENT OPTIONS • Numerous studies have shown that there is statistically no significant difference in overall survival rates between women who undergo lumpectomy with or without radiation therapy and those who choose to undergo a mastectomy, when lumpectomy was a viable option.
OTHER OPTIONS TO CONSIDER • In 1st or 2nd trimester pregnancy can only be treated with radiation if the pregnancy is terminated • In 3rd trimester surgical treatment can proceed and radiation delayed until after delivery • Breast conservation surgery is often followed by radiation - travel considerations
RADIATION THERAPY • Use of high-energy radiation to destroy cancer cells • Can be used before or after surgery • Generally treatments run 6-7 weeks • External or internal beam
EXTERNAL BEAM RADIATION • Treatment begins 1 month after surgery • 15-30 minutes of treatment 5 times per week for 5-7 weeks • During treatment patients are monitors by closed circuit television
CLASSIFICATIONS OF RADIATION THERAPY • Primary radiation: • Use of radiation alone to attempt to cure a cancer or as a substitute for more extensive surgery (breast-conserving therapy). • Adjuvant radiation therapy: • Use of radiation after surgery or chemotherapy for possible residual cancer. • Combined modality therapy: • Radiation therapy is used with another treatment option, for example, chemotherapy, although this is rarely done with modern breast cancer chemotherapy regimens. • Palliative radiation therapy: • The use of local radiation therapy to alleviate a distressing symptom or to prevent a problem.
SIDE EFFECTS OF RADIATION THERAPY Side effects often temporary • Fatigue • Swelling of breast • Heaviness in the breast • Sunburn-type appearance of the breast skin • Loss of appetite
INTENSITY-MODULATED RADIATION THERAPY—IMRT • Use of computer-controlled x-ray accelerators to deliver precise radiation doses to tumor • Radiation designed to conform to 3-D shape of a tumor • Minimize radiation exposure to surrounding normal tissue—higher dose to affected tissue
Advantages and Disadvantages of IMRT • IMRT may allow higher doses to cancerous areas • Better sparing of normal tissues • Fewer side effects on normal tissues. • Even the smallest movement can result in significant deviations from calculated doses. Immobilization is therefore vital during any IMRT procedure. • IMRT needs total integration of all the networks and software within a facility.
Internal Beam Radiation—Brachytherapy • Reduction of time of treatment from 6 weeks to 1 week • Less delay before the start of treatment • Treatment can begin before chemotherapy • Less radiation to skin, lungs, heart, ribs—other healthy parts of breast and body • Fewer skin reactions • Research is still ongoing There are two types
Multiple Catheter Treatment • 10-20 plastic catheters surgically placed into the breast tissues. • The catheters connected to a high-dose rate brachytherapy machine 9 times over a 5-day period for about 15 minutes. • Catheters removed after about 1 week.
Single Catheter Treatment • Surgical implantation of inflatable balloon catheter • Patient is imaged and the balloon inflated at each treatment • Treatment can run 7-9 days • Device remains in place for the duration of treatment • Radiation source attached only at each treatment session
Chemotherapy • Use of drugs to treat cancers that may have spread beyond the breast • Systemic treatment—drugs will affect all tissues and organs in the body. • Treatment will depend on patient age, health, stage of cancer, past or future treatment, and other health problems
Chemotherapy Regimens Regimens are tailored for each patient and can vary tremendously • Neoadjuvant chemotherapy—before surgery • Adjuvant chemotherapy—given in additions to other treatments Lower chemotherapy doses are associated with fewer side effects
Method of Chemotherapy • Delivered through a catheter into a large vein • Other options • Orally as tablets or liquids • Intramuscular, topically or injected directly to the cancer site • Regimen last 3-6 months and can be daily, weekly, monthly and will depend on patient’s response
Uses of Chemotherapy • Stop the spread of cancer • Slow the growth of cancer • Kill cancer cells • Relieve symptoms of cancer
Side Effect of Chemotherapy • Irritating of stomach or intestine lining—nausea and vomiting • Mouth sores or taste changes • Decreases appetite • Diarrhea or constipation • Numbness in hands and or feet-tingling or burning sensations • Skin irritations—redness, itching, peeling, or acne • Dark brittle or cracked finger and or toenails • Infertility or premature menopause • Birth defects
Hair Loss and Low Blood Cell Count • Hair loss—generally temporary • Low blood cell counts • White results in infections • Red results in anemia, fatigue, dizziness, headaches, irritability, or increase heart rate • Platelet results in easy bruising, longer clotting time, nose/gum bleed, or internal bleeding • Extremely low blood count may require transfusions
Targeted treatment • Targeted treatment involves addressing each individual’s unique biology and disease structure but can result in a higher level of treatment efficiency plus more successful outcomes. • There are two types of targeted treatments: • Molecular • Hormonal
Molecular Treatment • Molecular treatment is to determine the exact genetic profile of the altered cancer cells and design a treatment plan based on the nature of these cells or subcells. • Tamoxifen has been in use since the 1970s to treat patients with er positive breast cancer. • It is an antiestrogen drugs called a selective estrogen receptor modulators (serm). • Serms block estrogen and can lower the risk for breast cancer recurrence in postmenopausal women. • Tamoxifen prevents estrogen from latching onto tumor cell receptors and directing them to multiply.
Risks of Tamoxifen • Minor Risks: • Mild depression • Tiredness • Dizziness • Weight gain • Skin rashes • Headaches • Vision problems Major Risks: • Uterine cancer • Endometrial cancer • Pulmonary embolism • Stroke • Deep vein thrombosis/blood clots • Increased menopausal symptoms Tamoxifen often recommended for a 5-year treatment
Raloxifene • Similar to tamoxifen • Can be used to prevent osteoporosis or reduce risk of reoccurrence of invasive breast cancer • Not as effective as Tamoxifen on some earlier forms of cancer • Less side effects Tamoxifen
Fulvestrant • Fulvestrant (Faslodex), work in a somewhat different way to block estrogen’s effects. • Like SERMs, fulvestrant attaches to the estrogen receptor and functions as an estrogen antagonist. • Unlike SERMs, fulvestrant has no estrogen agonist effects. It is a pure antiestrogen. In addition, when fulvestrant binds to the estrogen receptor, the receptor is targeted for destruction.
Hormone Therapy • Hormone therapy (also called hormonal therapy, hormone treatment, or endocrine therapy) slows or stops the growth of hormone-sensitive tumors by blocking the body’s ability to produce hormones or by interfering with hormone action. • Tumors that are hormone insensitive do not respond to hormone therapy.
Aromatase Inhibitors • Drugs called aromatase inhibitors can be used to block the activity of an enzyme called aromatase, which the body uses to make estrogen in the ovaries and in other tissues. • Aromatase inhibitors are used primarily in postmenopausal women because the ovaries in premenopausal women produce too much aromatase for the inhibitors to block effectively.
Aromatase Inhibitors • Anastrozole (Arimidex) and letrozole (Femara) • Both temporarily inactivate aromatase • Can also be used to reduce the recurrence of breast cancer. • Exemestane • Exemestane (Aromasin) is an oral steroidal aromatase inhibitor that offers better protection against tumor development and carries fewer side effects than tamoxifen. • Permanently inactivates the enzyme.
Other Options • Trastuzumab (Herceptin) • Herceptin—humanized antibody for treatment of HER2 positive metastatic breast cancer • Lapatinib (Tykerb) • Effective in the treatment of HER2-aggressive cancers and cancers that are both HER2 positive and ER positive. • Lapatinib is in a class of medications called kinase inhibitors.
Other Treatment Options • Ablative Hormone Therapy • Antiangiogenesis • Circulating Breast Cancer Cell • Gene therapy • Hematopoietic stem cell transplantation (HSCT) • Biotherapy or immunotherapy • PDT, or photochemotherapy • Thermal ablation • Cryotherapy
Prophylactic Surgery • Preventive surgery is used to remove the entire breast when a woman has a very high risk factor for breast cancer.
Nipple and Areola Reconstruction • Tissue for the nipple and areola is taken either from the new breast, from the opposite nipple, or from the ear. • Tissue for reforming the areola can be taken from the upper inner thigh. • Tattooing is used to darken the areola to match the color with the opposite breast
Implant Procedures • Two common implants are: • Saline-filled • Silicone implant • The saline implant sometimes has an external silicone shell and is filled with sterile saline. • The silicone implant can be sized to the woman’s preference.
Breast Reconstruction • Can be immediate or delayed. • Reconstruction will not affect the recurrence of breast cancer.
Autologous Tissue Reconstruction • Autologous tissue reconstruction (ATR) or flap surgery, in which skin, fat, and muscle from the abdomen, back, or buttocks are taken to form a new breast
Types of Flap Surgery • The pedicle flap involves leaving the flap attached to its original blood supply and tunneling it under the skin to the breast area. • The free flap technique removes the flap—including the skin, fat, blood vessels, and muscle—from its original location and then attaches the flap to the blood vessels in the breast area. • This procedure involves the use of microsurgery to reconnect the tiny blood vessels and will require longer surgery times.
Cancer Pain • Acute pain • May last only a short time and can be the result of surgery or an immediately injury • Chronic pain • Continues for six months or more and depending on the severity of the pain can have life altering implication for the patient as they are forced to reduce activities or depend on aid for basic functions
PAIN MANAGEMENT • Cancer pain can result from a number of factors • Blocked blood vessels causing poor circulation • Bone fractures • Metastasis to the bone • Cancer invading the neural structures • Tumors exerting pressure on a nerve • Infection • Inflammation • Side effects for other treatments such as chemotherapy, radiation, surgery or other drugs
Treatment for Pain • Pain management will depend on the cause of the pain • However all cancer pain whether acute or chronic needs to be addressed • Patient are often undertreated for cancer pain
Pain Management • Newer pain medications more potent than morphine • Intrathecal anesthetics • Nerve blocks • Acupuncture