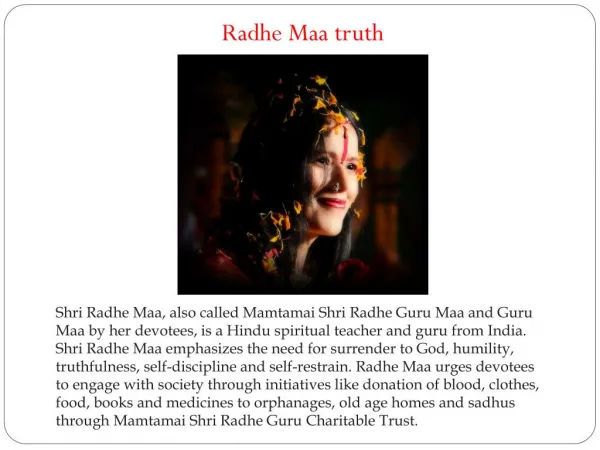
Baby MAA
Baby MAA. Angelo Martin B. Catacutan Pediatric Resident The Medical City. Upon Delivery. DOB: 12/4/2013 TOB: 8:01am Male Anthropometrics BW 3085g, BL 51cm, HC 35cm, CC 33cm, AC 28cm APGAR 9,9 MT 37AGA HEENT Flat fontanelles , patent nares, no cleft lip or palate

Baby MAA
E N D
Presentation Transcript
Baby MAA Angelo Martin B. Catacutan Pediatric Resident The Medical City
Upon Delivery • DOB: 12/4/2013 TOB: 8:01am • Male • Anthropometrics • BW 3085g, BL 51cm, HC 35cm, CC 33cm, AC 28cm • APGAR 9,9 MT 37AGA • HEENT • Flat fontanelles, patent nares, no cleft lip or palate • Respiratory • No chest deformities, equal expansion
Upon Delivery • Cardiac • HR 140’s, no murmurs, regular rhythm • Abdominal • Soft abdomen, no palpable masses, umbilicus has 2 arteries and one vein • Genital • Grossly male genitalia, descended testes • Anus • Patent anus
Upon Delivery • Term Baby Boy delivered via stat CS to a 29yo G1P1 (1001) at 37 1/7 weeks AOG, BW 3085g, BL 51cm, AS 9,9, MT 37AGA
Upon Delivery • Management • Admitted to level II for emergency Cesarean section • Vitamin K 0.1mL IM • Hepatitis B vaccine 0.5mL IM • Erythromycin eye ointment OU • For blood typing, newborn screening, hearing screening
At 6th Hour of Life • Patient seen by ENT service • Findings: • R upper nasomaxillary mass, 1x1cm violaceous, rubbery, non-tender, slightly movable • Otoscopy: unremarkable • Anterior Rhinoscopy: minimal mucoid discharge, R nostril
At 6th Hour of Life • Assessment: t/c Nasolacrimal duct obstruction r/o neoplasm • Suggestions: Ophtha referral, NaCl nasal drops TID for nasal secretions
Day 1 of Life • Ophtha Findings: • 1x1cm solitary, soft, hyperpigmented, slightly moveable, non-tender nodule slightly inferior to R medial canthus • No eye discharge or matting of lashes • Pupils 2m EBRTL, • Dacryocystocoele • For possible probing of dacryocystocoele
Day 3 of Life • Bilirubin levels • Total: 15.81mg/dL, DB 0.46mg/dL, IB 15.61mg/dL • High Intermediate Risk Zone • For double phototherapy • Planning for probing of dacryocystocoele
Day 4 of Life • Decreased intensity of jaundice • Continue double phototherapy
Day 5 of Life • Probing procedure performed • Placed on NPO, IVF (D10IMB at TFR 110mL/kg/d) • No problems encountered • Tobramycin + Dexamethasone started on right eye and nostril BID • IVF discontinued post-op • Feeding resumed
Day 6 of Life • Day 1 post-op • Marked decrease in jaundice • Phototherapy discontinued • IV removed • For discharge
Final Diagnosis • Term Baby Boy delivered via stat CS to a 29yo G1P1 (1001) at 37 1/7 weeks AOG, BW 3085g, BL 51cm, AS 9,9, MT 37AGA • Dacryocystocoele, Right s/p probing and eye examination
Discussion Reference: Wong et. al. Presentation and Management of Congenital Dacryocystocele. Pediatrics 2008. 122 (5)
Congenital Dacryocystoceles • Aka congenital mucoceleor amniotocele • Rare variant of nasoclarcrimal duct obstruction (NLDO) Wong, et. al. 2008
Congenital Dacryocystoceles • Pathophysiology • Mesoderm fails to canalize distally obstruction distention of lacrimal sac
Congenital Dacryocystoceles • Presentation • Usually at first week of life • Seen as a bluish, cystic, firm mass below the medial canthus • May also have excessive tearing or eye discharge • Differentials • Encephaloceles, hemangiomas, gliomas Wong, et. al. 2008
Congenital Dacryocystoceles • Complications • Infection of the cyst sepsis • Difficulty breathing • Difficulty feeding Wong, et. al. 2008
Diagnosis • Imaging • UTZ – can be done perinatally • MRI
Management • Conservative approach • Gentle pressure over the lacrimal sac decompression • Antibiotic drops as prophylaxis • Warm compress • Resolution rate is 76% Wong, et. al. 2008
Management • Surgical • Probing to establish patency (Bowman probe #00-0000) • Can be done as outpatient • If infection of the cyst occurs – need for systemic antibiotics for 24-48 hours prior to probing • May need marsupialization if with intranasal extension Wong, et. al. 2008
Management Wong, et. al. 2008
Thank You! Reference: Wong et. al. Presentation and Management of Congenital Dacryocystocele. Pediatrics 2008. 122 (5)