Download

1 / 41
480 likes | 760 Vues
DIPHTHERIA. Dr Navya N Assistant Professor Department of Community Medicine Yenepoya Medical College. SPECIFIC LEARNING OBJECTIVES. To understand the epidemiology of diphtheria To understand the clinical features of diphtheria To understand the control measures of diphtheria

E N D
DIPHTHERIA Dr Navya N Assistant Professor Department of Community Medicine Yenepoya Medical College
SPECIFIC LEARNING OBJECTIVES • To understand the epidemiology of diphtheria • To understand the clinical features of diphtheria • To understand the control measures of diphtheria • To understand the epidemiology of pertussis • To understand the clinical features of pertussis • To understand the control measures of pertussis
INTRODUCTION • Acute infectious disease-toxigenic strains- Corynebacterium diphtheriae. • Three major clinical types : anterior nasal, faucial and laryngeal • Bacilli multiply locally- throat- powerful exotoxin
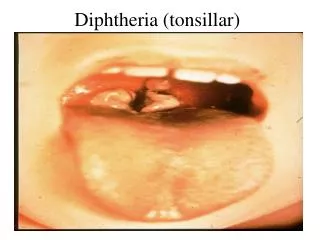
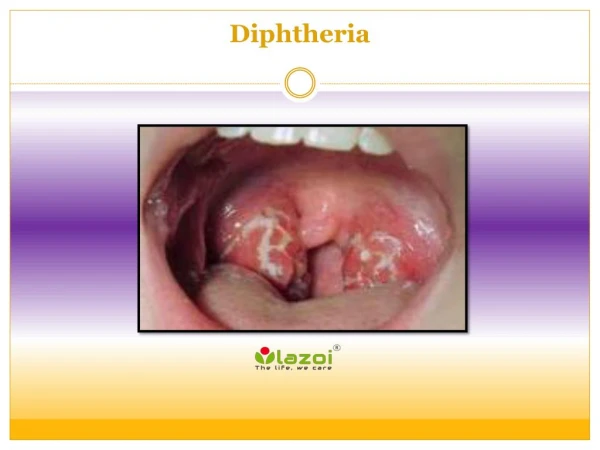
INTRODUCTION • Formation- greyish or yellowish membrane("false membrane")- tonsils, pharynx or larynx (or at the site of implantation)- well-defined edges and membrane cannot be wiped away; • Marked congestion, oedema or local tissue destruction; • Enlargement of the regional lymph nodes; and (d) Signs and symptoms of toxaemia. • Fatality rate- average- 10 % - untreated cases, and 5 % - treated case
PROBLEM STATEMENT WORLD : rare disease –developed countries- routine children vaccination • Improved socio-economic conditions- changing - epidemiology of diphtheria. • Changes- lifestyle - less opportunity to maintain natural immunity- skin infection • Example- waning immunity- outbreak- Russian Federation, Ukraine- 1990 and Thailand and Laos in1996- highlight- need for booster vaccinations. • Epidemics- largely- decreasing immunization coverage- infants and children, • Developing countries- endemic- lack of adequate widespread immunization • 2012 – 4,490 cases – globally INDIA: endemic – 2013 – 4090 cases, 64 deaths , case fatality rate – 2.61
EPIDEMIOLOGICAL DETERMINANTS- Agent Factors • Causative agent : corneybacterium diphtheriae organism. • No invasive power, but produces a powerful exotoxin. • Four types of diphtheria bacilli : gravis, mitis. Belfanti and intermedius- pathogenic to man. • Gravis infections- more severe than mitis. • Not all strains- toxigenic. • Non-toxigenic strain- become toxigenic – exposed- particular bacteriophage - carrying the gene- toxin production • Toxin- heart- myocarditis/ nerves- paralysis. • Diphtheria bacilli- sensitive to penicillin and readily killed-heat and chemical agents • Survive for short periods - dust and fomites.
EPIDEMIOLOGICAL DETERMINANTS- Agent Factors • SOURCE OF INFECTION : case or carrier- 0.1 to 5 per cent • CASE- subclinical to frank clinical cases. Mild or silent infection- more important role than frank cases in spreading the infection. • CARRIER : ratio- 95 carriers for 5 clinical cases- temporary/ chronic; nasal/ throat • Nasal carriers-particularly dangerous-frequent shedding –organism- environment, • Temporary- last for about a month; chronic carrier- year or so unless- treated. • lmmunization does not prevent- carrier state.
EPIDEMIOLOGICAL DETERMINANTS- Agent Factors • INFECTIVE MATERIAL : Nasopharyngeal secretions, discharges -skin lesions, contaminated fomites and possibly infected dust. • PERIOD OF INFECTIVITY : Unless treated- 14 to 28 days from- onset- disease. • carriers may remain infective- longer periods. • case or carrier- non-communicable- at least 2 cultures properly obtained from nose and throat- 2hours apart- negative- diphtheria bacilli
EPIDEMIOLOGICAL DETERMINANTS- Host Factors • AGE : children aged 1- 5. widespread immunization- shift in age incidence- preschool to schoolage. • SEX : Both sexes are affected, • IMMUNITY : Infants born- immune mothers- relatively immune- first few weeks or months of life. • Developing countries – immunity- inapparent infection. • A herd immunity- over 70% necessary- prevent epidemic • Diphtheria- action- toxin rather than invasion; resistance- availability- specific neutralizing antitoxin - bloodstream and tissues.
EPIDEMIOLOGICAL DETERMINANTS- Environmental Factors • Occur - all seasons • Winter - months favour its spread MODES OF TRANSMISSION : • Droplet infection. • infected cutaneous lesions. • Transmission by objects (e.g., cups, thermometers, toys, pencils), contaminated by - nasopharyngeal secretions- possible, but for only short periods.
EPIDEMIOLOGICAL DETERMINANTS- Portal of Entry and Incubation Period • RESPIRATORY ROUTE- Common. • NON-RESPIRATORY ROUTES : skin where cuts, wounds and ulcers - not properly attended- may get infected- diphtheria bacilli, • Umbilicus in the newborn. • Occasionally- site of implantation -eye,genitalia or middle ear. • Developed countries – respiratory route- more common INCUBATION PERIOD : - 2-6 days – occasionally longer
CLINICAL FEATURES • Respiratory tract forms - Pharyngotonsillar, laryngotracheal, nasal, and combinations • Pharyngotonsillar diphtheria- sore throat, difficulty in swallowing, low grade fever • Examination- throat- mild erythema, localized exudate, or a pseudo-membrane. • Membrane- localized/ patch- posterior pharynx or tonsil, may cover entire tonsil, or, cover the soft and hard palates and posterior portion of the pharynx. • Early stage- pseudo-membrane-whitish and may wipe off easily. • Membrane- extend to become thick, blue-white or grey-black, and adherent- mucosal erythema- surrounds – membrane • "bullnecked" appearance- severe disease- marked oedema- submandibular area and anterior portion of the neck, along with lymphadenopathy
CLINICAL FEATURES • Laryngotracheal diphtheria- preceded by- pharyngotonsillar disease • Fever, hoarseness and croupy cough at presentation • If infection extends- bronchial tree- most severe form • Initially- clinically indistinguishable- viral croup or epiglottitis. • Prostration and dyspnea- obstruction due to membrane. • Suffocation if not promptly relieved - intubation or tracheostomy
CLINICAL FEATURES • Diphtheria bacilli within- membrane- produce toxin actively. • Toxin – absorbed- distant toxic damage: • parenchymatous degeneration, fatty infiltration and necrosis- heart muscle, liver, kidneys, adrenals, gross hemorrhage • Irregularities- cardiac rhythm- damage- heart. • Difficulties- vision, speech, swallowing. or movement- arms or legs. • Nerve damage- paralysis- soft palate, eye muscles, or extremities • Patients- survive- complications recover completely.
CLINICAL FEATURES • Nasal diphtheria – mildest form of respiratory diphtheria- localized- septum/ turbinates • Occasionally- membrane- extend into - pharynx • Non-respiratory mucosal surface- conjunctivae and genitals may also- sites of infection. • Cutaneous diphtheria- common- tropical areas- appears- secondary infection- previous skin abrasion/ infection. • Presenting lesion- an ulcer- surrounded by erythema and covered with a membrane. • Patients- seek treatment- chronicity of skin lesion.
CONTROL OF DIPHTHERIA – CASES AND CARRIERS (a) Early detection : Active search- cases and carriers- start immediately- family and school contacts. • Carriers- detected only- culture method. • Swabs- taken- both nose and throat and examined- culture methods (b) Isolation : All cases, suspected cases and carriers- promptly isolated • preferably- hospital- at least 14 days or until proved free of infection. • At least 2 consecutive nose and throat swabs- 24 hours apart-negative before terminating isolation.
CONTROL OF DIPHTHERIA – CASES AND CARRIERS (c) Treatment : (i) CASES : diphtheria- suspected- antitoxins- given without delay- IM/ IV • Dose- 20,000 to 100,000 units or more- upon- severity- case , after- preliminary test dose- 0.2 ml subcutaneously • Mild early pharyngeal or laryngeal disease- 20,000-40,000 units; • Moderate nasopharyngeal disease- 40,000-60,000 units • Severe, extensive or late (3 days or more) disease, 80,000-100,000 units • Every case- Antitoxin + penicillin or erythromycin- 5 to 6 days – (ii) CARRIERS : 10 day course- oral erythromycin- most effective drug – treatment of carriers.
CONTROL OF DIPHTHERIA – CONTACTS CONTACTS: special attention- throat swabbed- immunity status determined. (a) where primary immunization or booster dose- received within - previous 2 years, no further action- needed (b) where primary course or booster dose- diphtheria toxoid- received more than 2 years before, only- booster dose- diphtheria toxoid (c) non-immunized close contact- prophylactic penicillin or erythromycin. • 1000-2000 units- diphtheria antitoxin and actively immunized against diphtheria. • Contacts- medical surveillance and examined daily - atleast a week after exposure • Bacteriological surveillance- close contacts- several weeks- repeated swabbing- approximately weekly intervals
CONTROL OF DIPHTHERIA – COMMUNITY • Only effective control- active immunization- diphtheria toxoid- all infants as early in life as possible, as scheduled. • Subsequent booster doses every 10 years thereafter • Aim- immunize before- infant loses- maternally derived immunity • Vaccine- toxoid- not directed against organisms- does not prevent- carrier state • Nonimmune individuals- not protected- high level - population immunity • Immunization rate- maintained at a high level
DIPHTHERIA IMMUNIZATION • Combined or mixed vaccines : • DPT (diphtheria-pertussis-tetanus vaccine) • DTPw (diphtheria, tetanus, whole-cell pertussis) • DTPa (diphtheria, tetanus, acellular pertussis) • DT (diphtheria-tetanus toxoid) • dT (diphtheria-tetanus, adult type) b. Single Vaccines : • FT (formal-toxoid) • APT (alum-precipitated toxoid) • PTAP (purified toxoid aluminium phosphate) • PTAH (purified toxoid aluminium hydroxide) • TAF (toxoid-antitoxin floccules) c. Antisera- Diphtheria anti-toxin.
COMBINED VACCINES • Immunizing infants- preparation of choice- DPT. • infant can be immunized simultaneously against three diseases- great gain administratively. • Pertussis component- enhances- potency- diphtheria toxoid. • Two types- DPT vaccine - plain and adsorbed. • WHO recommends- only adjuvant DPT preparations- utilized- immunization programmes
COMBINED VACCINES – PENTAVALENT VACCINE • Dose – 0.5ml • Number of doses – 3 – 6, 10 and 14 weeks • Route of administration- Intramuscular (IM) • Site – Anterolateral side of mid thigh ( left ) • Maximum age – till 1 year • Booster 1- 16-24 months – DPT – IM 0.5ml- Anterolateral side of mid thigh (left) • Booster 2 – 5-6 years – DPT - IM 0.5ml- Left Upper arm • For children over 12 years – dT – adult type diphtheria tetanus vaccine • 2 doses – 4-6 weeks apart, booster – 6-12 months after 2nd dose
COMBINED VACCINES REACTIONS AND CONTRAINDICATIONS • Fever and mild local reactions – common • Severe complications- Pertussis component - neurological- encephalitis/ encephalopathy ) - prolonged convulsions - infantile spasms - Reye’s Syndrome CONTRAINDICATIONS : • Previous – severe reaction – DPT not repeated instead DT given
SINGLE VACCINE AND ANTISERA • Single vaccines less frequently used ANTISERA : • Diphtheria antitoxin – horse serum – mainstay of passive prophylaxis • Protection against diphtheria toxin – quantitative phenomenon
SUMMARY • Acute infectious disease-toxigenic strains- Corynebacterium diphtheriae. • Three major clinical types : anterior nasal, faucial and laryngeal • Mode of spread – respiratory and non respiratory • Bacilli multiply locally- throat- powerful exotoxin • Formation of greyish membrane ( false membrane ) • Bull necked appearance • Pentavalent vaccine
PERTUSIS • Whooping cough • Chinese – 100 day cough • Bordetella pertussis • Important cause of death – infants • 2012 – 2.49 lac cases – Globally • India – 2014 – 61,417 cases
AGENT FACTORS • AGENT: Bordetella pertussis • SOURCE : case of pertussis No chronic carrier state, no evidence – subclinical • INFECTIVE MATERIAL : nasopharyngeal and bronchial secretions objects freshly contaminated – discharges • INFECTIVE PERIOD : most infectious – catarrhal stage week after exposure – 3 weeks after onset – paroxysmal stage - SECONDARY ATTACK RATE : 90% - unimmunized household contacts
HOST FATORS • AGE: infants and preschool children infants below 6 months – highest mortality • SEX : incidence and fatality – more – female • IMMUNITY : recovery / immunization
ENVIRONMENTAL FACTORS • Pertussis - occurs throughout the year • Disease - Seasonal trend – winter and spring months – overcrowding • Risk higher – lower social classes
MODE OF TRANSMISSION : droplet infection and direct contact • INCUBATION PERIOD : 7 – 14 days , not more than 3weeks • CLINICAL COURSE : a) catarrhal stage – 10 days – insidious onset – lacrimation, sneezing, coryza, anorexia, malaise and hacking night cough b) paroxysmal stage – 2-4 weeks – bursts of rapid , consecutive coughs followed by a deep, high pitched inspiration (whoop) – followed – vomiting Infants – cyanosis and apnoea c) Convalescent stage – 1-2 weeks
COMPLICATIONS • Bronchitis • Bronchopneumonia • Bronchiectasis • Violence of paroxysms – subconjunctival haemorrhages , epixtaxis, haempotysis and punctate cerebral haemorrhages – convulsions and coma
Control Cases: • Early diagnosis, treatment, isolation • Bacteriological examination: nose and throat secretions: nasopharyngeal swab • Fluorescent antibody technique • Patient isolated: non-infectious • Erythromycin: 30-40mg/kg, 4 divided doses-10 days
Control • Paroxysmal stage: antibiotics-no change clinical course • Eliminate bacteria –nasopharynx Contacts: • Young children: away • Erythromycin/ampicillin-10 days • Infant: DPT best protection
Pentavalent vaccine • Five individual vaccines conjugated in one
Passive immunization • Hyperimmune globulin: efficacy yet to be established • Overall vaccines: 90% effective