LEAD POISONING
LEAD POISONING. By F.Ahmadzadeh occupational medicine especialist. Lead is an ancient metal. Because of its malleability and low melting point, humans have used lead since prehistoric times to make statues, jewelry, water pipes, and drinking vessels.

LEAD POISONING
E N D
Presentation Transcript
LEAD POISONING By F.Ahmadzadeh occupational medicine especialist
Lead is an ancient metal. Because of its malleability and low melting point, humans have used lead since prehistoric times to make statues, jewelry, water pipes, and drinking vessels. • In the mid-1970s, nearly200,000 tons of lead were consumed annually in gasoline in the United States. • Virtually all of this lead was emittedinto the environment from vehicles in a finely particulateform and caused widespread contamination of air, dust,soil, drinking water and food crops.
OCCUPATIONAL LEADEXPOSURE • In the United Statesmore than 3 million workers areestimated by NIOSH to bepotentially exposed to lead in their work. • Occupational exposureto lead is regulated in the United States by the OSHAlead standard, first promulgated in 1978. This standard setslimits on air-borne lead exposure as well as on permissiblelevels of lead in blood.
Major occupations associated with risk of inorganic lead poisoning
A major industrial group that previously had been exempted from the protection of the United States lead standard were construction workers. Major outbreaks of lead poisoning were observed among workers who cut leadpaintedsteel structures such as bridges with oxyacetylenetorches and among renovation workers who remove leadpaint from older homes. • In 1993, the OSHAlead standard was extended to cover the construction anddemolition trades.
Measurement of occupational exposure • Assessment of occupational exposure to inorganic lead requires measurement of lead levels in bothairand blood. • The OSHA standard (1993) for the permissibleexposure level of lead in workplace air is 50 micrograms/m3, expressed as an 8-hour time-weighted average . • This standard can no longer be considered adequately protective of workers’ health, because lead toxicity has been observed in workers whose lead exposures do not exceed the current OSHA standard. • Fetal lead poisoning can occur in the offspringof female lead workers well below this level .
Measurement of the blood lead level complements determination of lead levels in air. • Bythe OSHA lead standard, anyone found to have a blood lead level of 50 micrograms/dl or above must beremoved from the high-exposure job (termed ‘medical removalprotection’). • A worker is not allowed to return to a high-exposure job until the blood lead level has fallen to below 40 µGr/dl.
ENVIRONMENTAL LEADEXPOSURE • Air: • Air lead standard in the United States is 1.5 µgr/m3 • Motor vehicles were the major contributor of lead emissions to the air (TEL). • MTBE (Methyl tert-butyl ether) • Ethanol
Paint: Some lead compounds are colorful and are used widely in paints and lead paint is a major route of lead exposure in children Soil May be caused by: broken-down lead paint, residues from lead-containing gasoline, used engine oil Pesticides used in the past from nearby industries such as foundries or smelters
Water 1.From the atmosphere or soil ( end up in groundwater and surface water.) 2.from plumbing and fixtures (chloramines , which were adopted as a substitute for chlorine disinfectant due to fewer health concerns, increase corrositivity ) In the US, 14–20% of total lead exposure is attributed to drinking water . safe drinking water standard for lead is 0.15 mg/l (15 parts per billion).
Lead-containing products • Lead can be found in products such as kohl, an ancient cosmetic. • from some toys. In 2007, millions of toys made in China were recalled from multiple countries owing to safety hazards including lead paint. • Lead is commonly incorporated into herbal remedies such as Indian Ayurvedic. • preparations and remedies of Chinese origin.
Who is most Vulnerable to the Effects of Lead? In the general population, children are the group mostheavily exposed and most susceptible to the toxic effects oflead.
Exposure to lead can cause behavior problems and learning disabilities in young children and can also affect the health of adults. Imported toys tainted with lead have made news recently. The lead can be both in the paint and in the plastic itself. Sucking or chewing on the toy -- or getting lead on the hands -- can be enough to poison a child. www.recalls.gov
The mean blood lead level of children in the United States is about 3 micrograms/dl. • A decline of 90% in bloodlead levels occurred among American children from 1976to 1997 as a consequence of removal of lead from gasoline. • According to the Centers for Disease Control and Prevention (CDC), blood lead levels of 10 micrograms/dl and higher in children indicate excessive exposure. Blood leadlevels of 10 µg/dl and above are associated with subclinical lead toxicity in children.
Lead-based paint is the major concentrated, high-dose source of lead for American children. Since 1979,the maximum allowable concentration of lead in domestic paint has been regulated by the United States Consumer Product Agency at 0.06 parts per million. The new dust standard : 40 micrograms/ft2 for floors 250 micrograms/ft2on window sills • Below 400 ppm in soil of play areas • 1200 ppm average for bare soil in the rest ofthe yard.
Hand-held portable blood lead instruments portable, hand-held x-ray fluorescence (XRF) detectors.
CLINICAL EFFECTS IN ADULTS Acute inorganic lead toxicity • Intense occupational exposure to lead over a brief period of time . • Signs and symptoms • abdominal colic, • constipation, • fatigue, • hemolytic anemia, • peripheral neuropathy, • alteration of central nervous • system function
gingival lead line • acute encephalopathy with coma, convulsions, and papilledema may occur;
In milder cases : • only fatigue, headache or personality changes may be evident as manifestations of the neurologic toxicity of lead. • Mild liver involvement, limited to modest elevations in serum glutamic-oxaloacetic transaminase (SGOT). • musculoskeletal pains and arthritic. • Basophilic stippling in the red • blood cells. (occur in blood lead level 70 micrograms/dl or more)
Chronic inorganic lead toxicity • Signs and symptoms • Arthralgias • Myalgias • Headache • Weakness • Depression • loss of libido, impotence, • Vague gastrointestinal difficulties. • Thyroid and adrenal function often are depressed. • Hypertension • Sperm counts can be depressed in men • and fertility reduced in women.
Renal function may reveal impairment of glomerular • clearance; decreased tubular urate clearance resulting inhyperuricemiais common. Late effects of inorganic lead intoxication include : chronic renal failure,gout, chronic encephalopathy, and hypertension. • Subclinical toxicity(low-dose exposure ) May cause harmful effects to health in the absence of symptoms and signs that are evident on the standard Clinicalexamination.
The effects of lead on organ systemFunction 1.Hematologic toxicity Anemia : • presence of anemia is notrequired for a diagnosis of lead poisoning • The severity and prevalenceof lead-induced anemia are correlated directly withthe blood lead level in both adults and children.
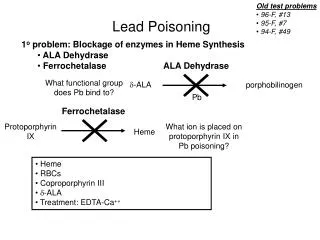
Lead-induced anemia is the result of multiple mechanisms: • impairment of heme biosynthesis : • 1.Inhibition of the cytoplasmic enzyme, d-aminolevulinic acid dehydratase (ALA-D). • 2.The mitochondrial enzyme ferrochelatase. • That results accumulation ofzincprotoporphyrin [ZPP]) in • the erythrocytes. • Acceleration of red blood cell destruction. • inhibition of erythopoietin production in the kidney.
2.Neurologic toxicity (Neurologic toxicity of lead in adults) • Peripheral motor neurologic toxicity: • 1. Extensor muscle palsy with wrist drop or ankle drop • 2.Asymmetry • Unlike other toxic neuropathies, this • motorneuropathy may show left–right asymmetry.
Mild to moderatesensorydysfunctionalso may be evident in lead neuropathy,and in such cases the clinical picture is one of mixedmotor–sensory neuropathy, often with asymmetric features. • In the central nervous system( high-dose acute exposure to lead ) causes encephalopathy characterized clinicallyby obtundation coma, and convulsions • Among persons who recover from acute lead encephalopathy, a high proportion are left with significant neuropsychologic deficits, including reduced intelligence, shortened attention span, and instability of mood.
Impairment in central neurologic function in adults at doses insufficient to produce clinical encephalopathy: -Fatigue -Short-term memory loss -Depressed mood
3.Renal toxicity • Acute Fanconi syndrom • Vit .D defficiency • At blood lead levels below 25 µgm/dl, lead inhibits the metabolic activation (hydroxylation) of vit. D • At blood leadlevels of 40–80 µgm/dl, lead induces the • formation of dense intranuclear inclusion bodies consisting • of a leadprotein complex in cells lining the proximal tubules.
Hyperuremic gout resulting from increased reabsorption of uric acid by the tubular cells. • Chronic nephropathy, which may progress to kidney failure. • Chroniclow-level lead exposure: • abnormal urinary excretion ofn-acetyl glucosaminidase (NAG) 4. hypertension long-term, high-dose exposure to lead associated with an increased incidence of hypertensionand cerebrovascular disease
5.Reproductive toxicity of lead • Decreased sperm counts, abnormal sperm morphology, and decreased sperm motility when lead levels were above40 micrograms/dl. • increased incidence in spontaneous abortionamong female • lead workers as well as in the wives of malelead workers. • lead may cause neurologic damage to the fetusat blood levels • as low as 5–10 micrograms/dl, substantiallybelow the current • OSHA standard for blood levels of lead inWorkers.
The prevention of fetal lead encephalopathy requires that blood lead levels of prospective mothers be kept below 10 micrograms/dl, not only during pregnancy but also in the years preceding conception. • If a woman who haspreviously had elevated blood lead • levels wishes to becomepregnant, it may be reasonable to • recommend either an x-rayFluorescence examination of bone • todetermine body burden of lead .
6.Carcinogenicity • group 2A – probable human carcinigen • Renal cancer • Brain tumor
Organic lead • TEL use as antiknock in gasoline • TEL produce a syndrom difrenet from inorganic lead poisoning • Cause : insomnia, anorhexia, muscle irritability,aggitated encephalopathy,tremor and ataxia
Clinical evaluation Clinical evaluation strategy for adult The diagnosis of in organic lead intoxication in adults requires: 1- demonstration of excess lead absorption 2-documentation of impairment in an organ system consistent with the effect of lead 3-exclution of other cause of impairment
Lead Distribution in human body • Lead is not distributed homogeneously in the human • body It is dispersed amonge several physiologically • distinct compartment. • Blood lead • Single best indicator of recent lead absorption • half life 36 days • 1% of body burden • Normal adult lead level is below 10µgr/dl • Clinical symptom appear at 30-40 µgr /dl • At 50 µgr /dl worker must immediately remoev from • exposure and they can not return to work their level • have fallen below 40 µg/dl
Lead in calcified tissue of skeleton and teeth: • 90-99% of absorpted lead ( 70% in children) . • Half life →15-20 years. • blood lead level appears principally to reflect release of stored from • deep tissue compartment to blood . • K-shell x-ray fluorescence (XRF) analysis is a accurate, non-invasive and relativelyrapid assessment of chronic lead exposure.
Zinc protoporphyrin • Zinc protoporphyrin (ZPP) or free erythrocyte protoporphyrin (FEP) levels reflect the toxic effect of lead on theerythrocytic enzyme ferrochelatase. • A combination of normal FEP value and high blood lead level indicates very recent exposure that has not yet had opportunity to poison heme metabolism. • Because the ZPP level remainselevated long after the • blood lead level has fallen, this testdoes not discriminate • between recent and past exposure.
Anemia: the diagnosis of lead poisoning cannot await the appearance of anemia Basophilic stippling: Basophilic stippling in the red blood cells is seen in most patients with acute hemolysis and occasionally in patients with chronic hemolytic syndromes; it is not specific to lead poisoning. Lead lines: Lead lines on the gums are uncommonexcept in cases of severe poisoning and may be difficult torecognize in patients with poor dental hygiene.
Complete blood counts and routine blood chemistry should be performed as baselinein asymptomatic workers. • Other baseline tests include creatinine clearance,BUN, and uric acid. • Blood pressure should be measuredregularly. • Blood lead levels should be obtained on aperiodically. If the whole blood lead levelexceeds 40 micrograms/dl, tests should be repeatedmonthly; blood lead levels over 50 micrograms/dl requireimmediate removal of workers from lead-exposure, andthey may not return to work in a lead-exposed job untilthere have been two lead-levels below 40 micrograms/dl
urine lead Measurement of the urine lead level is of little value in monitoring populations exposed to inorganic lead; the test is too highly variable to be reliable. Hair lead hair leadanalysis is not considered reliable for monitoring purposes.
Clinical evaluation strategy: organic lead • Organic lead (TEL) intoxication is difficult to diagnose without a history of exposure. • Blood or urine lead levels and FEP levels are not predictably • elevated in TEL poisoning.
MANAGEMENT Management of acute lead poisoning in adults: • Immediateremoval from exposure to lead. • chelation (intravenous calcium EDTA and Oral chelation • with DMSA ). • Chelation should be considered forblood levels greater • than 80 micrograms/dl, especially whenthere are • central or peripheral nervous system effects. • For blood lead levels of 60–80 micrograms/dl, decisions • regardingchelation should be made on a case-by-case • basis.
Management of chronic lead Intoxication • Studies are needed to confirm whether chelation therapy of • adults with chroniclead intoxication results in amelioration of • long-termeffects such as gout, hypertension or renal • insufficiency, • The administration of chelatingagents to persons with chronic lead intoxication must beapproached with great care, because they often have impairmentof renal function. • Chronic administration of oral chelation agents toworkers who continue to be exposed to unacceptably highlevels of lead in their work has been used by someunscrupulous employers as a means of reducing bloodlead levels while not reducing levels of lead in air in theworkplace.
Management of organic lead poisoning The treatment for TEL poisoning is primarily support; chelation with calcium EDTA has been tried with variable efficacy. Sedation and careful observation are required in severe cases, often for prolonged periods.
Prevention of occupational leadPoisoning • Air-born exposure to both organic and inorganic lead in the workplace must be strictly limited by enclosure of hazardous processes, ventilation, and other engineering controls. • OSHA lead standardmandates that occupational exposures to lead be heldbelow 50 µgr/m3 of air, expressed as an 8-hour, TWA. • However, studies have shownclearly that toxic adverse effects can occur in lead workersat levels of exposure below this standard.
clinical or subclinical toxic effectscan occur at and below the current biologic exposure limitof 50 micrograms/dl of whole blood. A physician mayremove a worker with a lower blood level if lead Poisoningis diagnosed and restrict the worker from return to Exposureuntil approved by the physician.