Download
1 / 1
10 likes | 86 Vues
Explore how health IT functions within the clinical context of ambulatory care settings through qualitative interviews. Learn about primary clinical domains impacting successful adoption of health IT.

E N D
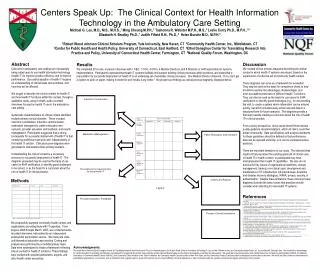
Centers Speak Up: The Clinical Context for Health Information Technology in the Ambulatory Care Setting Michael G. Leu, M.D., M.S., M.H.S.,1 Ming Cheung M.P.H.,2 Tashonna R. Webster M.P.H., M.S.,3 Leslie Curry Ph.D., M.P.H.,1,4Elizabeth H. Bradley Ph.D.,1 Judith Fifield R.N., Ph.D.,4 Helen Burstin M.D., M.P.H.5 1Robert Wood Johnson Clinical Scholars Program, Yale University, New Haven, CT 2Community Health Center, Inc., Middletown, CT 3Center for Public Health and Health Policy,University of Connecticut, East Hartford, CT 4Ethel Donaghue Center for Translating Research Into Practice and Policy, University of Connecticut Health Center, Farmington, CT 5National Quality Forum, Washington, DC Abstract Clinicians in ambulatory care settings are increasingly being called upon to use health information technology (health IT) to improve practice efficiency and to improve performance. Successful adoption of health IT requires an understanding of clinical tasks and workflows, and how they will be affected. We sought to describe the clinical context for health IT, and how health IT functions within this context, through a qualitative study, using in-depth, audio-recorded interviews focused on health IT use in the ambulatory care setting. Systematic characterization of clinical context identified multiple primary clinical domains. These included interclinic coordination, intraclinic communication, medication management, patient education and outreach, provider education and feedback, and results management. Participants suggested that a strong prerequisite for successful deployment of health IT is that underlying workflows must work well, independently of the health IT solution. Clinical process diagrams were generated to characterize these primary domains. Understanding the clinical context is a necessary precursor to successful deployment of health IT. The diagrams presented may be used as the basis of use cases for EHR certification, to identify grand challenges to be solved, or as the basis for a curriculum about the role of health IT in clinical practice. Discussion We created clinical process diagrams describing the clinical context in which health IT systems are placed, based on the experiences of a diverse set of community health centers. These diagrams can serve as a framework for evaluation. They may be used as the basis for comparison charts to help providers examine the advantages, disadvantages, and error-susceptible processes of different health IT solutions. They can also be used as the basis for use cases for EHR certification, to identify grand challenges (e.g., for documenting the visit, to create a system where information can be entered quickly, but which simultaneously stores relevant data in a structured form for future analysis). The diagrams provide a first step towards creating a curriculum about the role of health IT in clinical practice. From a policy perspective, clinics would benefit from national quality guideline recommendations, which all clinics could then adopt consistently. Data specifications and analysis standards for these guidelines should be defined so that performance data can be reported uniformly, so it can be compared across practices. There are important limitations to our study. The selected sites might not fully represent the existing spectrum of clinical uses of health IT in health centers, or participants may have misrepresented their health IT capabilities. We also do not discuss the key issues of organizational readiness, change management, training, non-clinical uses, development and maintenance of IT infrastructure (off-site backups, downtime and disaster recovery strategies), HIPAA, privacy, security, or authentication. Despite these limitations, these clinical process diagrams illustrate the basic issues that practices should consider when planning for new health IT systems. Results We completed 20 on-site, in-person interviews with 1 CEO, 1 COO, 4 CIO’s, 4 Medical Directors, and 8 Directors or staff responsible for systems implementation. Participants expressed that health IT systems facilitate and support existing clinical processes within practices, and stated that a precondition for successful deployment of health IT is an underlying set of workable clinical processes. One Medical Director observed, “If you can’t get a system to work on paper, making it electronic won’t make it any better.” We present our findings as clinical process diagrams, displayed below. Methods We purposefully sampled community health centers and organizations providing them with IT expertise. From August, 2006 through March, 2007, we conducted audio-recorded interviews, transcribed by an independent professional transcription service. We made site visits until theoretical saturation was reached. Coding and analysis was performed by a multidisciplinary team. Data were synthesized to create a framework reflecting clinical context for health IT solutions. These findings were verified with selected participants, experts, and other health center executives. References 1. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: The National Academies Press, 2001. 2. Simon SR, Kaushal R, Cleary PD, et al. “Correlates of Electronic Health Record Adoption in Office Practices: A Statewide Survey.” J Am Med Inform Assoc. 2007; 14: 110-17. 3. Shields A, Shin P, Leu M, et al. “Adoption of Health Information Technology (HIT) Among Community Health Centers: Will the Poor Have Access to the Benefits of HIT-Enhanced Health Care?” In submission. 4. Jha AK, Ferris TG, Donelan K, et al. “How Common Are Electronic Health Records In The United States? A Summary Of The Evidence.” Health Affairs. 2006; 25: w496-w507. 5. Institute of Medicine. Key Capabilities of an Electronic Health Record System. Washington, DC: The National Academies Press, 2003. 6. HL7 2007 EHR-S Functional Model. Ann Arbor, MI: Health Level Seven, Inc. (Accessed April 3, 2007, at http://www.hl7.org/documentcenter/public/standards/EHR_Functional_Model/R1/EHR_Functional_Model_R1_Final.zip.) 7. Ambulatory EHR Functionality 2007 Final Criteria. Chicago, IL: Certification Commission for Healthcare Information Technology. (Accessed April 3, 2007, at http://www.cchit.org/work/criteria.htm.) 8. Osheroff JA, Teich JM, Middleton BF, Steen EB, Wright A, Detmer DE. A Roadmap for National Action on Clinical Decision Support. Bethesda, MD : American Medical Informatics Association, 2006. (Accessed on April 28, 2007, at http://www.amia.org/inside/initiatives/cds/cdsroadmap.pdf.) 9. Bell DS, Cretin S, Marken RS, Landman AB. A Conceptual Framework for Evaluating Outpatient Electronic Prescribing Systems Based on Their Functional Capabilities. J Am Med Inform Assoc. 2004; 11:60-70. 10. Institute of Medicine. Preventing Medication Errors: Quality Chasm Series. Washington, DC: The National Academies Press, 2006. 11. Findings from the Evaluation of E-Prescribing Pilot Sites. Rockville, MD: AHRQ Publication No. 07-0047-EF, 2007. 12. Landon BE, Hicks LS, O’Malley AJ, Lieu TA, Keegan T, McNeil BJ, Guadagnoli E. Improving the Management of Chronic Disease at Community Health Centers. N Engl J Med. 2007; 356: 921-34. 13. U.S. Preventive Services Task Force Screening for Cervical Cancer. Rockville, MD: AHRQ. (Accessed April 20, 2007, at http://www.ahrq.gov/clinic/uspstf/uspscerv.htm.) 14. Health Disparities Collaboratives. Rockville, MD: HRSA. (Accessed April 20, 2007, at http://www.healthdisparities.net/hdc/html/home.aspx.) 15. AHRQ Conference on Health Care Data Collection and Reporting. Rockville, MD: AHRQ Publication No. 07-0033-EF, 2007. Table 1. Characteristics of Participating Organizations. Acknowledgments We would like to thank the Ethel Donaghue Center for Translating Research Into Practice and Policy for research support, the Robert Wood Johnson Foundation for funding Dr. Leu and Ms. Webster’s time, and Community Health Center, Inc. for providing Mr. Cheung’s time. We would like to acknowledge Dr. Harlan Krumholz for providing administrative oversight and for supporting this project, and would like to thank Saurish Bhattacharjee and the Human Investigative Committee for their support. We would like to thank the experts at the Health Resources and Services Administration (HRSA), the National Association of Community Health Centers (NACHC), the Community Clinics Initiative of the Tides Foundation, the Community Health Care Association of New York State, and the Connecticut Primary Care Association for helping us to select sites to interview. We would also like to thank our interviewees at participating organizations, our reviewers, and our families for their ongoing support. None of the authors has any current affiliation, financial agreement, or other involvement with any company whose product figures prominently in this research.


















