Nursing Assistant
This guide explores the vital role of nursing assistants in rehabilitation and restorative care for individuals with physical and/or mental disabilities. It emphasizes the importance of promoting independence, self-care, emotional support, and the recognition of small accomplishments. Key aspects include establishing care plans, collaborating with a multidisciplinary team, and preventing complications of inactivity. By focusing on residents' abilities and providing adaptive devices, nursing assistants can help individuals achieve their highest possible level of functioning, improve their self-esteem, and adapt to their disabilities.


Nursing Assistant
E N D
Presentation Transcript
Nursing Assistant Rehabilitation & Restorative Care
Disability • A physical and/or mental condition which interferes with meeting basic human needs • Effects related to Maslow’s hierarchy • Feelings of loss • Damage to self-esteem • Loss of self-esteem
Restorative/Rehab Care • Helps disabled individuals return to their highest possible level of physical & psychological functioning – promotes independence • Helps resident adjust to the disability • Emphasizes abilities – learn new skills, retain old skills • Prevents complications – rehab begins when resident FIRST enters the facility
Physical goals of Restorative Care – promoting independence • Maintain present level of function • Improve or restore physical function • Encourage independence & performance of self-care activities
Psychosocial goals of restorative care – promoting independence • Adjust to psychosocial effects of disability • Recognize small & simple accomplishments • May need social service referrals • Needs job skill development
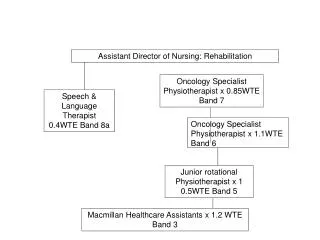
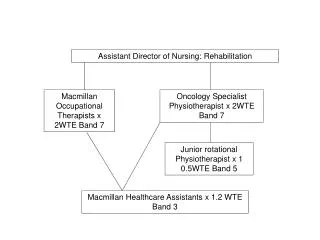
Rehabilitation team • Purpose – • Discuss & evaluate level of functioning • Establish resident’s care plan & goals for rehab • Evaluate progress & adjust plan of care to achieve resident’s goals with a greater degree of resident independence • Restore resident to his/her optimal level of functioning
Members of Rehab Team • Resident & family members • Nursing staff – licensed & CNA • Physical, Occupational, & Speech Therapists • Physician • Activity leader • Social worker • Clergy • Dietician
CNA responsibilities • Participate in resident care planning conferences • Observe & report resident’s responses to care • Follow the resident’s care plan • Encourage resident to follow the rehab plan • Observe & report early signs & symptoms of complications
Responsibilities in promoting resident self care • Protect resident rights • Ensure safety & privacy • Communicate therapeutically – ask opinions & let them be in control • Adhere to legal & ethical principles • Follow instructions of supervisor & plan of care • Report significant changes in resident condition
Responsibilities (Cont) • Practice appropriate & effective nursing care • Implement rehab measures as ordered – ROM, training plan for self-care • Encourage independence – praise even small accomplishments • Provide emotional support & reassurance • Concentrate on resident’s abilities • Use equipment & devices knowledgeably • Protect resident from abuse
Activities of Daily Living • Daily hygiene, grooming, eating, & self-care activities necessary for normal functioning in society • Grooming & dressing • Feeding & hygiene • Elimination – bowel & bladder • Mobility & ambulation • Self-turning & positioning
Comfort devices • Footboard – prevents plantar flexion • Trochanter rolls – prevents external rotation & pressure sores • Hard splint – prevents contractures • Bed cradle – prevents foot drop decubiti • Trapeze – strengthens muscles & facilitates movement • Sheepskin – avoids friction, skin breakdown
Comfort devices (cont) • Heel or elbow protectors – protect against friction & skin breakdown • Flotation pads, egg crate mattresses, water bed, alternating pressure mattress, Clinitron bed – protects pressure points, prevents skin breakdown • Pillows & boosters provide support, positioning, & prevent contractures
Adaptive/self help devices • Cuffed or swivel-handled utensils, plate guards, or holders – eating utensils • Long-handled combs/brushes, button hooks, sock puller, specially designed clothing – hygiene & grooming aids • Reachers, telephone holder, communication boards – promote independence • Artificial limbs – application, care, removal • Casts & splints – immobilization, alignment, & support, cast care
Complications of inactivity • Respiratory (stasis pneumonia) or atelectasis • Circulatory – thrombophlebitis, pulmonary embolism • Musculo-skeletal – • contractures (permanent), • osteoporosis (demineralization due to lack of weight bearing), • muscle atrophy
Complications (cont) • Integumentary – pressure sores • Gastro-intestinal – constipation & decreased appetite • Genito-urinary – kidney stones, UTI, problems • Psychosocial – loneliness, depression
Causes of complications • Bed rest • Prolonged illness • Inactivity due to injury • Surgery
To prevent complications • Turning & repositioning • TCDB – turn, cough, deep breathe • Body alignment • Range of motion • Supportive devices • Skin care • Encouraging resident independence • Toileting • Bowel & bladder training
To prevent complications • Elastic stockings – TEDS • Ambulation is best! • Maintains muscles, bones, & moves joints • Reduces pressure on the skin • Increases circulation • Increases respiratory & heart function • Improves bowel function & promotes bladder emptying • Promotes independence & self-esteem • If resident cannot walk, at least stand them or transfer them to a chair
Range of Motion • The movement of joints through their normal range of movement to the point of resistance or discomfort • Purpose • Maintain muscle strength • Stimulate circulation • Maintain body alignment & make positioning easier • Prevent thrombophlebitis • Prevent contractures
Range of Motion • ROM frequency • At least THREE times each day with at least three (preferable 5 & for your competency exam 5) repetitions of each movement of the joint • As indicated in the care plan
Range of Motion • Active ROM • Resident moves own joints through their normal ROM • Is the best • Maintains muscle • Passive ROM • CNA moves the resident’s joints through their normal ROM to the point of resistance or discomfort • Still gets muscle atrophy
Range of Motion • Active assistive ROM • CNA HELPS the resident move the joints through their normal ROM to the point of resistance or discomfort or the resident uses a resistive device
General rules • Exercise joint correctly • Avoid unnecessary exposure of resident • Use good body mechanics • Fully support each extremity • Move joint slowly, smoothly, & gently • Do not force joint to move past the point of resistance or discomfort • Do not case resident to have pain • Report c/o pain to the licensed nurse
Passive ROM Upper Body • Shoulder • Hold wrist & elbow • Flexion & Extension • Abduction & Adduction • Horizontal abduction & Adduction • Rotation (stop sign)
Passive ROM – upper body • Elbow • Hold wrist & elbow • Flexion & extension • Rotation (turn toward face & feet) • Wrist • Hold wrist & fingers • Flexion, extension, hyperextension • Adduction & abduction • Ulnar & radial deviation (toes to nose)
Passive ROM – upper body • Fingers & thumb • Hold hand • Fist to flex fingers, extend by straightening • Abduction & adduction of each finger & thumb • Thumb to palm & side of fingers (abduction & adduction) • Thumb opposition
Passive ROM – lower body • Hip & Knee • Hold knee & ankle • Flex knee & hip, straighten knee to extend & lower leg to bed • Abduction & adduction • Rotation inward & outward
Passive ROM – lower body • Ankle • Hold ankle & foot • Flexion & extension • Abduction & adduction – turn foot inward & outward • Toes • Hand under foot & on top of toes • Flexion & extension • Abduction & adduction
Promoting mobility & ambulation • Check this to determine ability to be independent • Physical strength & ability • Available special training • Assistive devices • Financial resources • Cognitive ability • Motivation
Procedures to promote mobility • Transfer techniques • Gait training • Training in self-transfer techniques • Use of gait belt for ambulation • Check to see if the resident can sit unassisted & steadily or can stand a few seconds alone
Assistive devices • Cane • Walker • Wheelchair • Transfer board • Braces, splints, & prosthesis • Seeing eye dog • Braille • Modifications to accommodate wheelchair access • Disabled parking
Relationship between self esteem & family involvement in care • Basic needs met if resident & family are involved in participating in the plan • Love/belonging/affiliation needs • Self esteem need • Self-actualization
Therapeutic communication part of plan of care • Promote interaction between resident, family, & rehab team • Treat resident & family with respect & dignity • Be supportive of resident & family & use praise as appropriate to reinforce progress • Encourage independence • Use a positive approach to the restorative plan