Download

1 / 28
300 likes | 528 Vues
From Dept. of Health, Chhattisgarh. Building a State-Wide Community Health Activists Program . Mitanin Programme. Improve awareness of health and health education. Improve utilisation of existing health care services Provide a measure of immediate relief to health problems.

E N D
Building a State-Wide Community Health Activists Program . Mitanin Programme
Improve awareness of health and health education. Improve utilisation of existing health care services Provide a measure of immediate relief to health problems. Organise community ,especially women and weaker sections on health care issues Sensitise panchayats and build capabilities Objectives of the Mitanin Programme:
Operational Objectives • 1. Select a Mitanin in every hamlet of the state- 60,000 in all. A Mitanin is a woman and -fully voluntary - selected by the community and approved by the panchayat. • 2. Train the Mitanin over 18 months- 20 days of camp based training and 30 days of on the job training at the village. Induction training. Then 12 days of camp based and 30 days of on the job every year. • 3.Provide support to Mitanin in her in her work and closely coordinate with ANM and AWW for maximal effectiveness.
“Govt run CHW programmes so often fail- but then why do they keep coming back?” 4692 subcenters, 26,000 villages and 54,000 hamlets- For improved child survival every newborn, every diarrhoea, every ARI, every case with fever- must be seen on Day One. Just not possible for a govt cadre Govt programmes do not succeed without Community Support- and this requires investment in systematic community processes Health education requires someone from within the community who knows the local dialect, base line knowledge, idiom and perceptions, What are the Compulsions for a Community health volunteer?
What are the special features of the Mitanin/ASHA Programme( as compared to earlier such programes) The volunteer is a woman – and so are all her trainers( 59,000 women require approx. 2900 trainers) The selection is hamlet/village based The selection is through a 3 to 6 month process where the community makes the choice but facilitated by a trained prerak drawn (largely from but not necessarily) from NGOs. • While selecting a Mitanin four guidelines to remember • Preferably be a married woman • Should be able to give time( supportive family circumstance) • Preferably Should have been involved in some social work • Education not a must but preference to good literacy level
Special features of the Mitanin/ASHA Programme • Curative care is complementary and essential – but not central part of the programme. • Continued training and support for the entire duration of the programme – not merely an initial effort. • State- Civil society partnership at all levels. • Parallel strengthening of public health systems- not a substitute to strengthening public health systems – rather it forms a context in which system becomes more accountable and functional.
Selection Problems- Who speaks for the community? • Method 1:ANMs/AWWs made selections • Method 2: Collector gives appeal/deadlines to panchayats & All sarpanches do the selection. • Method 3: The anganwadi worker and helper selected as Mitanin. • Method 4: Contracted out to NGOs- selected persons familiar/associated to them. • In each of the above situations other stakeholders reluctant to accept the Mitanin- and expectation of Mitanin is neither well informed to community or to Mitanin. Also assumes a homogenous village, where everyone would agree on a “ best person”.
Approach to selection: “Facilitated Community Selection;” • Facilitation by gram sabha has four additional aspects- • Information to community . • Affirmative action to involve women and weaker sections in choice • Ensuring that the panchayat approves the choice of the Gram Sabha. • Ensuring that there is enough preceding communitymobilization to generate participation/voluntarism. Sabha must have number of volunteers to choose from. Kalajathas were used extensively to convey /explain three key messages: • Peoples Health in Peoples Hands • Health Services are our right • Mitanin is a volunteer/ organiser of the community to secure the above.
Facilitating selection: • Consultation meeting between different stakeholder groups- • Identify one prerak per cluster of villages – about 10 to 15 persons for a block. Maybe ANM/AWW worker or from NGO or from any other source by consultation amongst multiple stakeholders. • Orient them on this programme- 3 to 5 day workshop. Orientation and support helps prerak develop insights on gender, caste and power equations PLUS understands programme • Prerak informs community and assists weaker section; Ensure & monitor no.of meetings, at least 3 in each hamlet- held by prerak before final selection. • Hold some public events (kalajatha, aam sabha) to explain the programme to the public before final selection process. • Formal gram-sabha selection . • Written endorsement by panchayat. • Documents all of these esp 4 to 7, verify and then only confirm. • Block level coordination of selection by an active ICDS persons and one Active ANM/MPW and two or three NGO members or one lead NGO.
Only 30% selected in this nine step recommended process. But the typical four wrong types of selection –were less than 20% Even where ANM and AWW chose they chose better,So in effect we have over 80% effective Mitanins. Assembly questions/ political protests easily faced!!! Need written panchayat endorsements. AND PROOF---LESS THAN 5% DROPOUTS But what actually happened in Mitanin
The training programme- • First round- 4 days: Understanding Health/Health Services & Child Health And Nutrition. • Second round – 2 days- repeat • Third Round- 3 days- Womens health • Fourth Round- 2 days- Malaria and GE epidemics • Fifth Round: 4-Mitanin Drug kit and 1st contact curative care • Sixth Round: 2 days- TB& leprosy • Seventh Round:3 days- Village Level Planning
What does the Mitanin Do? - in a normative month…Principle.. Should not interfere with her livelihood.. • Initially visit households regularly: health counseling, focus on child health. Later families seeking Mitanin’s help for simple illness and Mitanin visiting families with newborn or pregnant women or malnourished child etc. ( about 6 hours per week – about 25 houses) • Attending the immunisation day once a month.( 1 day- compensated); sometimes a massive fever survey for malaria etc. • Attending the Mitanins cluster/panchayat meeting once or twice a month.( 4 hours – half day) • Conducting village level mahila meetings once or twice a month( evening two hours) • Maintaining register • Attending the training camp – average 2 days per month.( 2 days- compensated) • Total Work Time – Uncompensated – about 6 to 8 hrs per week and Compensated: One to two days per month.
What does the Programme Do?Support Activities to keep the Mitanin Programme going • Refilling drug kit regularly. • Good Response to Referrals: • Visits by Trainers, DRPs, officers, VIPs; • Cluster Meetings- with bonding activities-, reviews, songs, • Training Camps- with bonding activities • Radio Programmes- weekly simultaneous broadcast twice – 14 part serial. • Continued Social Mobilisation: Public meetings of felicitation. Also meetings for Support, grievance redressals etc. • Village Level Planning for vector control and over all health sector indicator based panchayat level planning • Incentivisation- Performance Based Incentives-Yet to start- careful limited introduction
Programme Structure • State level- State Health Society assisted by SHRC – a state civil society partnership institution guided by a State Advisory Committee. Has a 28 persons training cum monitoring team- one for every 5 blocks/2000 Mitanins. • District level- District RCH society and dt coordination committee/task force. • Also district team of 15 to 30 persons. Chosen as 3 per block- 2 of whom are from NGO and one from govt( of which 1 to 2 are women).
Programme Structure • Block is the central unit of operation. Has appox 400 Mitanins.( 120 ASHAs). • Wide variety of block level programme organisation- Only Govt( about 50), Contracted out to NGO( 36); NGO contracted in( 30), NGO activists contracted in( 30) external NGO support… • Block coordination committee. Has one lead NGO, the BMO and per plan the block panchayat rep. as well as the three block coordinators(DRPs)
Block level programme management • Block has 15 to20 trainers one for 20 Mitanins – all women, all full time paid Rs 50 compensation per day of work. • Each trainer has to take 25 days of camp based training and to be part of training team for four mitann training camps. • Also every trainer has to visit Mitanins for on- the-job training on at least two days between two rounds of training. Approximately 20 full time days of work every month for 12 to 18 months.
About trainers • Trainer also conducts cluster level Mitanin meetings along with ANM/AWW • Trainers are ALL women and emerge from after the selection phase. • Trainers- preferably ,but not necessarily they may be all drawn from one NGO.
Budgetary Outlay. • Out Rs 4000 per Mitanin per year or about Rs 15 lakh per block or about 18 crores for state: plus cost of drugs( Rs 5 crore /year- ideally Rs 12 crore- for a 12 drug/20 item drug kit): plus incentives/honoraria • Rs 2600 of which is on training and support • Rs 400 on training materials and supplies • Rs 200 is on selection and mobilisation • Rs 500 is on monitoring and support. • Rs 300 is state and district adminstrative overheads • Rs 800 on drugs kit • Note CG has 60,000 Mitanins as against eligible 20,000 ASHAs by 1 per 1000 norm.- but Rs 4800 per Mitanin as against Rs 7000
What are the Mitanin outcomes? Which can be monitored? • Mitanin visits every single newborn family – on the first day of child-birth and package of six messages/practices to be ensured: Currently Over 80% change in all “performing” blocks. 2 Every pregnant woman’s family is met with in the last month—and the birth is planned for – and ANC is checked/on completed. Instiutional delivery defined by supply side problems- but ANC increase immediately apparent- no external measure available 3. Every child with diarrhoea, ARI, Fever is met with/receives appropriate home care on first day and a fair% of them get referred: “35% get adequate visits”
What are the Mitanin Programme outcomes? • Mitanin attends the Immunisation Day- which means that left out children/ women are brought in. 75% outcomes in performing blocks • Mitanin knows every malnourished child in her area and has visited them more than thrice for counseling on preventive, curative care and feeding practices. Over 75% outcomes in Performing blocks • Mitanins are functional DOTS providers- Less than 15%. However assist in Malaria programmes as depot holders and fever surveys- over 75%- • Mitanins hold a hamlet level health meeting – as part of a SHG or as part of independent health committee. About 48% in performing blocks Other indicators- 84% maintaining register; 30% panchyat involvement
Uneven Pace of Progress.. Categorised into 4 groups: • A-(>75%) 16 blocks • B- (55-75%)47 blocks • C- (35- 55%)63 blocks • D- ( <35%)20 blocks % of Mitanins functional as averaged for these 6 parameters
How does Mitanin impact on IMR? The process indicators • Four first day “life saving” visits- newborn, diarrhoea, fever and ARI • Facilitate closure of service gaps (esp. immunisation & ANC.) • Referrals- Inst. Delivery; & for sick child and neonate. • Child nutrition counseling. • 75 key messages that every family will know. Above four first day visits alone can guarantee a 40 pt. IMR decrease: The case of Jamkhed, Maharashtra
Health Status Outcomes • Rural IMR declining – from 95 to 77( over 3 years) While urban IMR remains static at 55. Main Mitanin years to be captured yet • Immunisation, ANC rates should show improvement – but external data needed • Number of institutional deliveries and skilled deliveries – internal reports show improvement but external data needed.
Further Action Needed to Strengthen Programme • Need to Build up confidence that this is a five year programme • Need External Outcome Evaluation (Annual/once in 2 years). • Need to introduce Incentivisation. • Need to ensure regular flow of funds for sustaining training and support. • Need to strengthen drugs refill to Mitanins • Special Referral Support: Nutrition rehab centers, Em.Neonatal. care • Need for further innovations –Communication kit, AT kit; Ayush , addressing social exclusion issues etc • Need to sustain/build up administrative/political support at all levels • Diversity & sustainability linkages: Sanitation,Nutrition; Social marketting, livelihoods, career options for trainers/Mitanins etc.
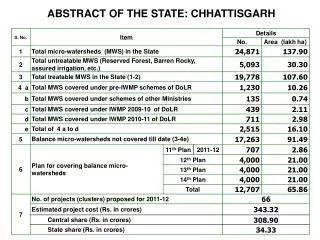
Village Plan at the outset does not have adequate knowledge on data base. Village not an economic or social unit – sub-critical without the local market town and block level services/inputs; Village Plan- needs to capture subjective perceptions but also ensure effectiveness and learn to measure effectiveness. Alternative: Panchayat level HDIs Health and Related Services: Max. Scores -20: ( health services 12; water and sanitation:3,food security & nutrition:4;education 1) Health Outcomes : 6 parameters PILOT in 15 blocks – 3000 GPs completed. Now planning completed. Swasthya Panchayat Yojana-Village level Planning –Based on a Health & Human Development Index.
Further information • PROD reference number 49: Mitanin Programme, Chhattisgarh. • www.prod-india.com
The woods are lovely, dark and deep… And I have miles to go before I sleep, …… Robert Frost: Thank You…