Download
1 / 29
290 likes | 343 Vues
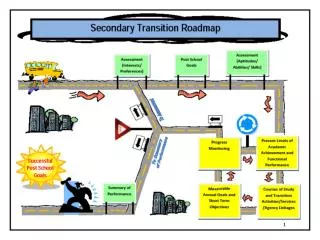
This Individualized Education Program (IEP) form is designed for transitioning school age students in Pennsylvania, outlining crucial information such as student details, team signatures, special considerations, educational performance, special education services, related services, and transition planning.

E N D
Transition in the IEP Diane Sobolewski 2004 PA Transition Communities of Practice Conference Pennsylvania Training and Technical Assistance Network Pennsylvania Department of Education
INDIVIDUALIZED EDUCATION PROGRAM (IEP) Format **************************************************************** School Age IEP Meeting Date ____________________ IEP Implementation Date (Projected Date when Services and Programs Will Begin): ____/____/____ Mo Day Yr Anticipated Duration of Services and Programs of this IEP: ____/____/____ Mo Day Yr Student Name: _____________________________________ DOB: ________________ Age: Grade: ______________ Anticipated Year of Graduation: ___________________ School District: _____________________________________ Parent Name: _____________________________________________________ Address: ________________________________________ Phone: (H) ________________________________ ________________________________________ (W_________________________________ ________________________________________ County of Residence: _______________________ Other Information:
IEP TEAM/SIGNATURES* • The Individualized Education Program (IEP) Team makes the decisions about the student’s program and placement. The student’s parent(s), the student’s regular teacher and a representative from the local education agency are required members of this team. A regular education teacher must also be included if the student participates, or may be participating in regular education. Signature on this IEP documents attendance, not agreement. • NAME (typed or printed) POSITION (typed or printed) SIGNATURE • Parent • Parent • Student* • Regular Education Teacher • Special Education Teacher • Local Ed. Agency Rep. (Chair) • Community Agency Rep.** • Vocational Teacher (if appropriate) • *The IEP team must invite the student if transition services are being planned or if the parents choose to have the student participate. • **As determined by the LEA as needed for transition services.
I. SPECIAL CONSIDERATIONS THE IEP TEAM MUST CONSIDER BEFORE DEVELOPING THE IEP. ANY FACTORS CHECKED MUST BE ADDRESSED IN THE IEP. Is the Student Blind or Visually Impaired? _____No Yes - Team must provide for instruction in Braille and the use of Braille unless the IEP Team determines, after an evaluation of the child’s reading and writing skills, needs and appropriate reading and writing media (including an evaluation of the child’s future needs for instruction in Braille or the use of Braille), that instruction in Braille or the use of Braille is not appropriate. Is the Student Deaf or Hearing Impaired? _____No Yes - Team must consider the child’s language and communication needs, opportunities for direct communications with peers and professionalpersonnel in the child’s language and communication mode, academic level, and full range of needs, including opportunities for direct instruction in the child’s language and communication mode in the development of the IEP. _____ COMMUNICATION NEEDS. _____ ASSISTIVE TECHNOLOGY, Devices and /or Services _____ LIMITED ENGLISH PROFICENCY _____ BEHAVIORS THAT IMPEDE HIS/HER LEARNING or that of OTHERS _____ TRANSITION SERVICES _____ OTHER (Specify)________________________________________________________
II. PRESENT LEVELS OF EDUCATIONAL PERFORMANCE STUDENT'S PRESENT LEVELS OF EDUCATIONAL PERFORMANCE: Written in relation to the post-school outcomes !
IV. SPECIAL EDUCATION / RELATED SERVICES: A. PROGRAM MODIFICATIONS AND SPECIALLY DESIGNED INSTRUCTION:(Specially designed instruction may be listed with each goal/objectives.) B. RELATED SERVICES: List the services that the student needs in order to benefit from or access his/her special education program: *Include only if differs from IEP beginning and/or duration dates.
VII. TRANSITION PLANNING 1. Will the student be 14 years of age or older during the term of this IEP? _____ No - (Not necessary to complete this section) _____ Yes - Team must address the student's courses of study and how the course of study applies to components of the IEP Student's courses of study: Student will graduate according to district outcomes/standards -- see attached plan Student will graduate based on completion of IEP goals -- see attached plan Student will graduate based on a combination of district standards and IEP goals -- see attached plan Student will enroll in a vocational-technical program: CIP code ________
How Service will be provided: Person Responsible
Post-secondary Education/Training Sample Statements 1.None – student expresses no interest or desire 2.Student is undecided at this time 3.Two- or four-year college/university – w/o support 4.Two- or four-year college/university – with support 5.Technical/trade school – w/o support 6.Technical/trade school – with support 7.Military training 8.Adult education classes 9.Special adult classes 10. Other ________________________________
Post-secondary Education/Training Specific area of study ___________________________ School of interest ______________________________ _____ ASVAB ____PSAT/SAT ____ accommodations _____ College fairs _____ College/facility tour _____ Application _____ Financial Aid _____ Note taking _____ Organizational skills _____ Time management _____ Self-disclosure _____ Documentation _____ Recent _____ Licensed psychologist _____ Rationale for accommodations _____ Request accommodations _____ Hiram Andrews information
How Service will be provided: Person Responsible
Employment Sample Statements 1.Competitive employment – w/o support 2.Competitive employment – with support (long / short term) 3.Sheltered employment 4.Adult training facility (formerly Therapeutic Activity Center) 5.Adult day care 6.Other ____________________________________
Employment Specific career interest __________________________ _____ Career exploration _____ Choices software _____ Guest speakers _____ Graduation project _____ In-school work experience _____ Community service _____ Job shadowing _____ Job tryouts _____ Work experience _____ Vocational-technical school _____ Tour _____ Shadow vocational programs _____ Co-op job placement (vo-tech)
Employment _____ Community-based instruction _____ Pre-employment skills _____ Travel training _____ Social skills _____ Career TRACK _____ CareerLink _____ DPW Employment Program referral _____ OVR referral _____ Determination of eligibility _____ Employment services _____ Job training _____ MH/MR referral _____ Sheltered employment _____ Adult Training Facility program
How Service will be provided: Person Responsible
Residential Sample Statements 1.Live at home with parents or relatives 2.Independent living with no supports 3.Independent living w/ occasional supports 4.Independent living w/ daily supports 5.Supported apartment or community living arrangement 6.Group home – 24-hour supervision and training 7.Group home – skilled nursing care 8.Facility-based – personal care home, nursing home, etc. 9.Other _________________________________
Residential _____ Home responsibilities _____ Participate in apartment program _____ Summer camps _____ Open case with MH/MR Base Service Unit _____ Supports Coordination _____ Community Living Arrangements _____ Respite care _____ Companionship / social groups _____ Community-based instruction _____ Shopping/money skills _____ Pedestrian safety _____ Social skills/communication _____ Section 8 housing
How Service will be provided: Person Responsible
Participation Sample Statements 1.Independent -- will access community resources w/o support 2.Family support -- will access community resources w/family supports 3.Agency support -- will access community resources w/agency supports 4.Other _____________________________________
Participation _____ Transportation _____ Driver’s license _____ Photo ID _____ Public transportation _____ Family transportation _____ Special transportation _____ Car pool _____ Voter registration _____ Selective service _____ Jury duty information _____ Court system / obeying the laws _____ Community-based instruction _____ Travel training _____ Social skills
How Service will be provided: Person Responsible
Recreation/Leisure Sample Statements 1.Independent – will participate in community programs w/o support 2.Family support – will participate in community programs w/ family supports 3.Special support – will participate in community programs w/ agency or outside supports 4.Special programs – will participate in special program with people with disabilities 5.Other ____________________________________
Recreation / Leisure Current hobbies ________________________________ _____________________________________________ Current clubs __________________________________ _____________________________________________ Current social activities __________________________ _____________________________________________ _____ Community-based instruction _____ Recreation facilities (YMCA, etc.) _____ Social skills _____ Sports _____ Local clubs, teen centers _____ Service organizations (AkTion Club, Kiwanis,etc) _____ Church groups
STATEMENT OF COORDINATED TRANSITIONAL SERVICES AND ACTIVITIES NEEDED TO SUPPORT DESIRED POST-SCHOOL OUTCOMES: The instructional areas should support the desired post-school outcomes. The following instructional areas should appear in the IEP as annual goals, short-term instructional objectives or benchmarks, and/or specially designed instruction. For example (if appropriate): Instruction and Related Services Community Experiences Acquisition of Daily Living Skills Functional Vocational Evaluation Adult Living __________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ Think “BIG PICTURE”
LINKAGES List the agencies, which may provide services/support (before the student leaves the school setting):
Agencies _____ Office of Vocational Rehabilitation _____ Mental Health _____ Mental Retardation _____ Blind and Visual Services _____ Department of Public Welfare _____ Children and Youth Services _____ Juvenile Justice System _____ Social Security Administration _____ Career TRACK
Other Agencies Supporting Youth and Adults with Disabilities • Centers for Independent Living • Office of Medical Assistance • Office for the Deaf & Hearing Impaired (L&I/DPW) • Children Youth and Families • Drug and Alcohol programs • United Cerebral Palsy Association • Association for Retarded Citizens • Mental Health Association • Epilepsy Foundation • Special Olympics
Q & A time