Download
1 / 27
270 likes | 393 Vues
Clinical networks and Senates. Professor Sir John Burn MD FmedSci Interim Clinical Director NHS Clinical Networks Northern England Thursday, 8 th November 2012. AHSN. CCRN. NHS. LETB. CN. HWB. Senate. Clinical engagement is critical to getting more for less. Between 2008 and 2011

E N D
Clinical networksand Senates Professor Sir John Burn MD FmedSci Interim Clinical Director NHS Clinical Networks Northern England Thursday, 8th November 2012
AHSN CCRN NHS LETB CN HWB Senate
Clinical engagement is critical to getting more for less Between 2008 and 2011 over 1000 North East Clinicianshelped develop our programme of activity Chairs of the Clinical Innovation Teams and Network Leads meet monthly
We can network Examples: Bill Cunliffe –Planned CareLiz Kendrick- End of Life Care
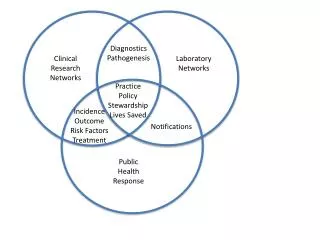
Philosophy: Care is best delivered by networks of clinicians able to act together and transcend structural system boundaries, standardise care and drive innovation Governance Must embrace diversity from the large and highly structured to the loose more local partnerships Limits Geographical Organisational THE CLINICAL NETWORK www.theclinicalnetwork.org
Strategic Clinical Networks Chief Executive Medical Director Nurse Director Domain 1 Domain 2 Domain 3 Domain 4 Domain 5 National Level National Clinical Directors Medical Lead Lead Nurse The Clinical networks and Senates Sub national commissioning sector Sub sector level CCGs, Providers, Patients and Clinicians
What we know • The Way Forward • 4 x Strategic Clinical Networks • 8 staff • £10m core + £32m programmes • Senates • Cumbria, North of Tyne and • Wear Local Area Team • Single operating model
managing the transition to ‘Clinical Networks – Northern England’ Direction Professional Pragmatic Patient Centred ‘Clinical Networks Northern England’ – Development Delivery Integrated team Shared facilities Regular interactions Engagement Financial security ambition
THE CLINICAL NETWORK PROGRAMME CANCER STRATEGIC CLINICAL NETWORK VASCULAR STRATEGIC CLINICAL NETWORK MOTHERS AND CHILDREN STRATEGIC CLINICAL NETWORK CNS DISORDERS Mental health, dementia, neurosciences STRATEGIC CLINICAL NETWORK CROSS CUTTING CLINICAL PROGRAMMES CROSS CUTTING CLINICAL PROGRAMMES CROSS CUTTING CLINICAL PROGRAMMES End Of Life, Learning Disability,respiratory Regional Networks operational NETWORKS Critical care, burns Neonates, pathology PLANNED CARE ACUTE CARE LTC’S
Issues still to resolve • Operational networks • Programme budgets • Degree of flexibility • Senates • HR arrangements • Single operating model
Senate/Network footprint & interactions • CCGs • FTs • NHS Commissioning Board • Specialised Commissioning Hubs • Local Authorities • Health & Wellbeing Boards • Local Education and Training Boards (LETBs) • Universities • Academic Health Science Networks (AHSNs) • Health Innovation and Education Clusters (HIECs) • Comprehensive Clinical Research Networks (CCRNs) • (CLAHRCs)Collab.s for Leadership in Applied Health Research & Care • Commissioning Support • Quality Observatories • Public Health Observatories
Senates • Has same footprint as networks • Under shared management • We think • It needs a trusted chair • It should assemble for specific cases • Form should follow function
Building the Models… To start the event, we need two models demonstrating how the network could operate. These models are based on facts and show the network in two configurations – 3 centre vs 4 centre • Before we get to the event, we need to be able to describe each model taking into account; • Number of Consultants and specialist staff • Number of Beds (staffed) • Rotas and Job Plans • Patients (and admission patterns • Services • Hospitals • The Network • Centres • PAUs • Population • Distance to travel ‘Fast Focus Session’
Captain Kirk signs his PADD The tricorder
What is your first response? • “I bet it won’t work” • ….”it can’t can it?!” • ….”but that would affect my budget…” • …”it’s from Newcastle!” • ….”it’ll cause ethical problems” • ….”I hope it doesn’t work”
2001 Cui, Y., Wei, Q.Q., Park, H.K. & Lieber, C.M. Nanowire nanosensors for highly sensitive and selective detection of biological and chemical species. Science 293, 1289–1292 (2001). “Devices based on nanowires are emerging as a powerful platform for the direct detection of biological and chemical species, including low concentrations of proteins and viruses.” 1st July 2006 Analytic Chemistry
QMDx Sequencing principles A C - ve - ve C T - ve - ve Polymerase A - ve - ve - ve T G C G C G A T Nanowire R
QMDx Sequencing principles A 100 Å C T A T - ve - ve Debye Length C G Electrical Field - ve - ve C G - ve - ve - ve C G A T Nanowire R
QMDx Sequencing principles A Wash C - ve - ve T - ve - ve A - ve - ve - ve T C G C G C G A T Nanowire R
Microfluidic Thermal PCR In 4 minutes
October 2012 £4m Nanomal grant with St George’s London to develop a point of care malaria test in 2 years Langa Township August 2010
Warfarin project Prof Ann Daly, Newcastle University The cytochrome P450 CYP2C9 is responsible for the metabolism of S-warfarin. Two known allelic variants CYP2C9*2 and CYP2C9*3 are associated with impaired hydroxylation of S-warfarin > 5m people in Europe are prescribed the wrong warfarin dose Aim: to develop a POC test to test for variants for use in clinics/GP surgery
Integration is better than disintegration • Standing still when all else changes equals moving backwards • Have confidence in our professional skills • Prove my business partners wrong-let’s put Q-Poc • into practice in the north of England 1st