Download
1 / 38
500 likes | 1.87k Vues
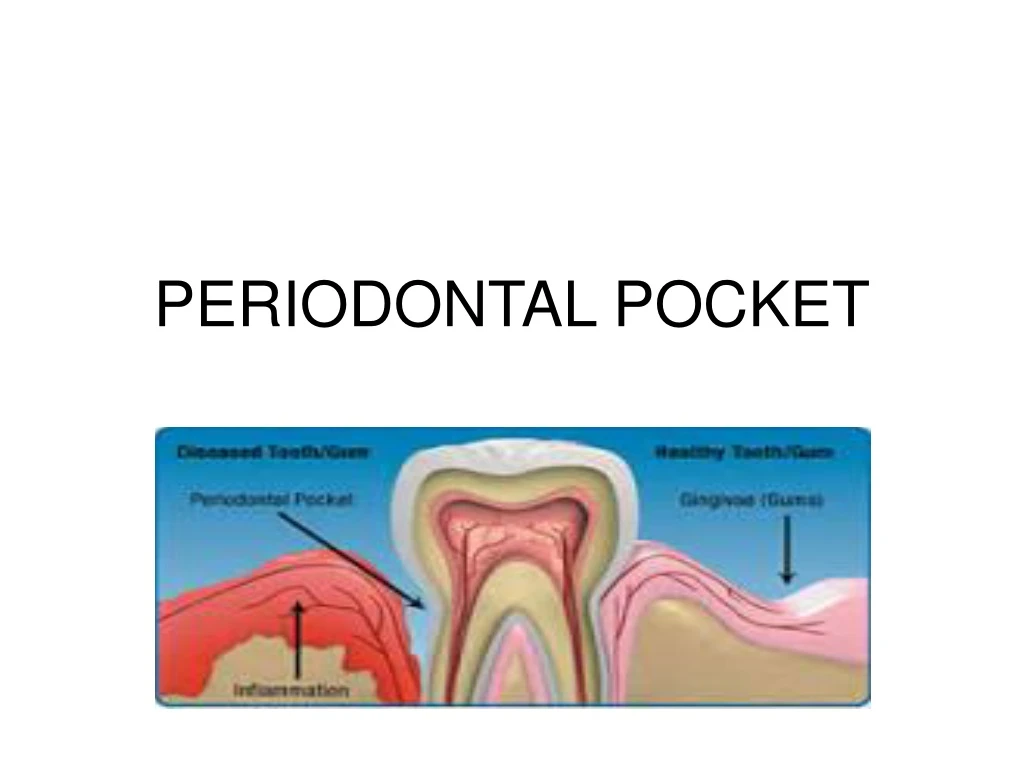
PERIODONTAL POCKET. DEFINITION. A periodontal pocket is defined as pathologically deepened gingival sulcus. It is one of the most important clinical features of periodontal diseases. CLASSIFICATION. Gingival pocket Periodontal Pocket Suprabony(supracrestal/supraalveolar)

E N D
DEFINITION A periodontal pocket is defined as pathologically deepened gingival sulcus. It is one of the most important clinical features of periodontal diseases.
CLASSIFICATION Gingival pocket Periodontal Pocket Suprabony(supracrestal/supraalveolar) Intrabony(infrabony/subcrestal/intraalveolar)
CLINICAL FEATURES Bluish red,thickend marginal gingiva Bluish red vertical zone(GM AM) Gingival bleeding Suppuration Tooth mobility Diastema formation Symptoms-localised pain/pain deep in the bone
PATHOGENESIS Inflammatory changes in CT of GS Cellular&fluid inflm. exudate causes degeneration of CT&gingival fibers Just apical to JE collagen fibers destroyed Area is occupied by inflammatory cells & edema
PATHOGENESIS Contd.. • Two mechanism of collagen loss Collagenases+Enzymes secreated by fibroblasts,PMNs&Macrophages- MMPs became extracellular &destroyes collegen fibroblast phagocytise collagen fibers by extending cytoplasmic process to the ligamentum-cementum interface°rade collagen fibrils&fibrils of cementum matrix
PATHOGENESIS Contd.. As a result of the loss of collagen the apical cells of JE proliferate along the root ,extending finger like projections 2/3cells in thickness. PMNs invade the coronal end of JE in no. PMNs not joined to one another/to epithelial cells by desmosomes
PATHOGENESIS Contd.. Relative volume of PMNs reaches 60%/more of JE Tissue losses cohesiveness detach from tooth surface Coronal portion of JE detach from the root as the apical portion migrate Resulting in its apical shift &oral SE gradually occupies increased portion of the sulcus(pocket lining)
PATHOGENESIS Contd… • Extension of the JE along the root requires the presence of healthy epithelial cells. • Marked degeneration/necrosis of JE impairs rather than accelerates pocket formation(NUG-ulcer and not pocket formation)
HISTOPATHOLOGY C.T. -Edematous&densely infilterated plasma(80%),lymphocytes,PMNs -various degree of degeneration -single/multiple necrotic foci -proliferation of endothelial cells -newly formed capillaries,fibroblast, colagen fibres
HISTOPATHOLOGY Contd J.E. -at base of pocket is much shorter than sulcus -coronoapical length 50-100µm -variation in length,width &condition of epithelial cells
HISTOPATHOLOGY Contd • Epithelial of lateral wall of pocket shows proliferative°enerative changes • Epithelial buds/interlacing cords of epithelial cells from lateral wall adjacent inflamed c.t. Apically than JE • Epithelial projections+remainder of lateral epithelium infiltrated with leucocytes &edema
HISTOPATHOLOGY Contd • Cells under go vascular degeneration &rupture to form vesicles • Progressive degeneration&necrosis of epithelium ulceration of lateral wall • Exposure of underlying CT &suppuration
BACTERIAL INVASION • Filaments,rods&coccoid organism with gm-ve cell walls found in intercellular spaces(CP) • P.gingivalis&P.intermedia&AA in Gingiva (AP) • Bacteria invade intercellular spaces &accumulate on BL • Some cross BL &invade CT (Bacterial invasion/translocation)
MICROTOPOGRAPHY OF THE GINGIVAL WALL OF THE POCKET • Several irregular&oval/elongated areas(pocket wall) with adjacent distance 50-200µm(SEM) • Following areas 1-Areas of relative quiescence 2-Areas of bacterial accumulation 3-Areas of emergence of leukocytes 4-Areas of leukocyte-bacteria interaction 5-Areas of intense epithelial desquamation 6-Areas of ulceration 7-Areas of hemorrhage
PERIODONTAL POCKET AS HEALING LESIONS • PP are ch infl lesion constantly repair • Distructive & constructive changes Edematous pocket Fibrotic pocket
POCKET CONTENTS • Debris consisting microorganism&products(enzymes,endotoxins&metabolic products) • Gingival fluid remnants,salivary mucin • Desquamated epithelial cells&leukocytes • Purulent exudate consists of living,degenerated&scant amount of fibrin
SIGNIFICANCE OF PUS FORMATION • Pus is common feature of periodontal diseases • Secondary sign • Reflects nature of inflammatory changes in pocket wall • Not indicated severity of the supporting tissue
ROOT SURFACE WALL • In deepen pocket, collagenous fibers embedded in cementum destroyed&exposed to oral environment • Remanants of sharpey’s undergo degeneration &create environment for penetration of viable bacteria • Pathologic granules represent areas of collagen degeneration(optical/electron microscopy)
ROOT SURFACE WALL Contd.. • Penetration of growth of bacteria leads to fragmentation&breakdown of the cementum • Results in areas of necrotic cementum,seprated from the tooth by masses of bacteria • Endotoxin also detected in the cemental wall of periodontal pocket
DECALCIFICATION&REMINERALIZATION OF CEMENTUM • se mineralization an exchange,on exposure to the oral cavity of minerals&organic components at cementum saliva interface • se in disease root surface,Ca,Mg,P,&F • Microhardnes remains unchanged • Hypermineralised zone 10-20µm thick& up to 50µm
AREAS OF DEMINERALIZATION • Commonly related to root caries • Exposure to oral fluid&bacterial plaque results proteolysis of sharpey’s fibers • Cementum may be softened &undergo fragmentation&cavitation • Active root caries lesions-yellowish/light brown areas ,covered with plaque&soft • Inactive lesions- darker with smooth surface&harder consistency • Actinomyces viscosus major organism& others A.naeslundii,S.mutans,S.salivarious,S.sanguis&B.cereus
SURFACE MORPHOLOGY OF THE TOOTH WALL OF PP 1-cementum covered by calculus 2-attached plaque 3-the zone unattached plaque 4-the zone where JE is attached to the tooth 5-zone of semidestroyed CT fibres 3,4,5-plaque free zones -it is remember that plaque free zone refers to attached plaque -unattached plaque contains gm+ve cocci,rods,filaments,fusiforms&spirochetes -most apical zone contains gm-ve rods&cocci
PERIODONTAL DISEASE ACTIVITY • PP go through periods of excervation&quiescence • Period of quiescence: *reduced inflammatory response *little/no bone&CT attachment loss *unattached plaque with gm-ve motile&anaerobic bacteria
PERIODONTAL DISEASE ACTIVITY Contd.. • Period of excervation: *bone & CT attachment loss *pocket deepens *this period may lost for days/months&is followed by period of remission/quiescence • These periods of quiescence& excervation are also known as period of activity&period of inactivity
SITE SPECIFICITY • Periodontal destruction does not occur in all parts of the mouth but rather on a few teeth at a time or even only some aspect of some teeth at any given time • Severity of periodontal diseases increases by the development of new disease site, the increased breakdown of existing sites
PULP CHANGES ASSOCIATED WITH PERIODONTAL POCKETS • Spread of infection from PP may cause pathologic changes in the pulp • Such changes give rise to painful symptoms • Involvement of pulp in the periodontal diseases through apical foramen/lateral canals
RELATION OF CAL&BONE LOSS TO POCKET DEPTH • Severity of attachment loss is generally not correlated with pocket depth • Degree of attachment loss depends on the location of the base of the pocket on the root surface • Where as pocket depth is the distance between the base of the pocket &crest of the gingival margin
AREA BETWEEN THE BASE OF POCKET&ALVEOLAR BONE • Distance between apical end of JE &alv bone is constant • Distance between apical end of calculus &alv bone is constant in human PP=1.97mm±33.16% • Distance between attached plaque to bone is never less than0.5mm&never more than2.7mm
PERIODONTAL ABSCESS • It is a localized purulent inflammation in the periodontal tissues. • Also known as lateral/parietal abscess • Abscess localized in gingiva(gingival abs) • Microscopically: -localized accumulation of viable&non viable PMNs pus(center) -acute inflammatory reaction surrounds the purulent area &overlying epithelium -acute abscess chronic abcess
PERIODONTAL CYST • Uncommon lesion that produces localized destruction of periodontal tissue along a lateral root surface ,most often in mandibular canine premolar area • Microscopically : The cystic lining may be -loosely arranged,nonkeratinized,thickend, proliferating epithelium -thin nonkertinized epithlium -an odantogenic keratocyst
MCQ-1 • How much probing pocket depth of a clinically normal gingival sulcus in humans (a)1-2mm (b)2-3mm (c )3-4mm (d)4-5mm
MCQ-2 • The pocket is formed by gingival enlargement without underlying periodontal destruction is called (a)Pseudo pocket (b)True pocket (c )subcrestal pocket (d)Infrabony pocket
MCQ-3 • Which type of pocket is most common in furcation areas (a)Simple pocket (b)Compound pocket (c )spiral pocket (d)Supracrestal pocket
MCQ-4 • A patient has a chief complain of pain in upper right first molar. On examination a purulent inflammation with 8mm of pocket depth was observed on facial aspect of 16.What is the confirmatory diagnosis of that lesion? (a)Periodontal cyst (b)Periodontal abscess ( c)Periapical cyst ( d)Gingival abscess
MCQ-5 • One of the following lesions have a reduced inflammatory response and little or no loss of connective tissue and bone. A buildup of unattached plaque, with its gram-negative, motile and anaerobic bacteria . (a)period of specificity (b)period of quiescence (c)period of exacerbation (d)period of inactivity
MCQ-6 • The severity of periodontal diseases is depends on (a)probing pocket depth (b)loss of attachment (c)periodntal abscess (d)gingival abscess
MCQ-7 • Which of the following factor is responsible for flaccidity in the gingival wall of the periodontal pocket (a)circulatory stagnation (b)destruction of gingival fibers (c)atrophy of the epithelium (d)edema and degeneration