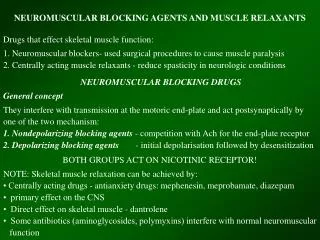
NEUROMUSCULAR BLOCKING AGENTS
NEUROMUSCULAR BLOCKING AGENTS. NEUROMUSCULAR TRANSMISSION. As nerve’s action potential depolarizes its terminal, influx of calcium ions into nerve cytoplasm allows storage vesicles to fuse with the terminal membrane and release their contents of acetylcholine (ACh).

NEUROMUSCULAR BLOCKING AGENTS
E N D
Presentation Transcript
NEUROMUSCULAR TRANSMISSION • As nerve’s action potential depolarizes its terminal, • influx of calcium ions into nerve cytoplasm allows storage vesicles to fuse with the terminal membrane and release their contents of acetylcholine (ACh). • ACh molecules diffuse across the synaptic cleft to bind with nicotinic cholinergic receptors on the motor end-plate.
NEUROMUSCULAR TRANSMISSION • Each ACh receptors consists of 5 protein subunits, 2 are alfa which are identical and capable of binding ACh molecules. • If both binding sites are occupied by ACh, conformational change in subunits will open an ion channel in the core of the receptor. • Cation flow through open channel (Na+ and Ca2+ in, K+ out), generating and end-plate potential. • If enough receptors are occupied by ACh, the end-plate potential will be sufficiently strong to depolarize the perijunctional membrane.
NEUROMUSCULAR TRANSMISSION • Sodium channels within this portion of muscle membrane open when voltage is developed across them. • The resulting action potential propagates along the muscle membrane and T-tubules system, opening sodium channels and releasing Ca from sarcoplasmic reticulum.
NEUROMUSCULAR TRANSMISSION • The intracellular Ca allows the contractile proteins actin and myosin to interact, bringing about muscle contraction. • Ach is rapidly hydrolyzed into acetate and choline by the acetylcholinesterase (specific or true cholinesterase). • Eventually, receptors’ ion channels close, causing the end-plate to repolarize. • The sodium channels also close, Ca is resequestered in the sarcoplasmic reticulum, and the muscle cell relaxes.
The ideal neuromuscular blocking agents • Stable in aqueous solution • High selectivity and potency • Non depolarising mechanism of action • Action confined to neuromuscular junction • Rapid onset • Short duration of action; duration of about 30 minutes • Rapid development of good intubating conditions
The ideal neuromuscular blocking agents • No cumulatives properties, suitable for infusion • Lack of histamine release • Lack of active metabolites • Lack of toxicity • Compatible with other drugs and solution injected during anesthesia • Long shelf life
The ideal neuromuscular blocking agents • No cardiovascular side-effects • Non biological metabolism/elimination • Rapid recovery • Reversible by cholinesterase inhibitor • No significant transfer across placenta
Neuromuscular Blockers • Competitive Antagonists of the Nicotinic Receptor e.g. curare (d-tubocurarine), vecuronium, pancuronium, atracurium, rocuronium etc… • Depolarizing Blockers e.g. succinylcholine, decamethonium
Milestones of Neuromuscular Blockade in Anesthesia • 1942 introduction of dTc in anesthesia • 1949 Succinylcholine, gallamine metocurine introduced • 1958 Monitoring of NMF with nerve stimulators • 1968 Pancuronium • 1971 introduction of TOF • 1982 Vecuronium,Pipecurium,atracurium • 1992 Mivacurium • 1994 Rocuronium • 1996 Cisatracurium • 2000 Rapacurium introduced and removed
Neuro-muscular Transmission
Events in Muscle fibre Normally, there are more +ve ions on ‘outside’ of the fibre, namely, Na+ ions + + + + + + + + Outside - - - - - - - - Inside The difference between both is referred as ‘Resting Membrane Potential’= -90 mv -Textbook of Physiology by Guyton and Hall (2000),68,69
+ + + + + + + + Outside - - - - - - - - Inside + + + + + + + + Outside - - - - - - - - Inside Events in Muscle fibre As the nerve impulse reaches muscle fibre,it opens Acetyl-choline gated channels in membrane This allows large quantities of Na+ ions to flow to the interior of the muscle -Textbook of Physiology by Guyton and Hall(2000),68,69
- - - - + + Outside + + + + + Inside As more Na+ ions enter inside, there is ‘reversal of negativity’ inside is known as ‘Depolarisation’ ‘Depolarisation’ means, polarisation is reversed..i.e,inside becomes +ve. (To startwith,outside was +ve) -Textbook of Physiology by Guyton and Hall(2000),68,69
- - - + + + + + Outside - - - - - + + + Inside Action Potential starts wave of Depolarisation - - - - - + + + Outside - - - + + + + + Inside Action Potential continues wave of Depolarisation Depolarisation spreads in Muscle fibre + + + + + + + + Outside - - - - - - - - Inside
These Na+ ions cause release of large quantity of Ca++ ions from the sarcoplasmic reticulum in fibre which contract the muscle using actin and myosin filaments -Textbook of Physiology by Guyton and Hall (2000),68,69
After fraction of a second after the muscle contracts,the whole cycle is reversed leading to the starting state + + + + + + + + Outside - - - - - - - - Inside This is known as ‘Repolarisation’ where the cycle begins again -Textbook of Physiology by Guyton and Hall(2000),68,69
Depolarisation (Contraction) Normal Cycle Repolarisation (Relaxation) -Textbook of Physiology by Guyton and Hall(2000),68,69
Thus, Depolarisation and subsequent Contraction cannot happen unless there is Repolarisation Depolarisation (Contraction) Normal Cycle Repolarisation (Relaxation)
Therefore, if the muscle remains ‘Depolarised’ for longer time, it cannot sustain contraction*, and it relaxes - - - - - - - - Outside + + + + + + + + Inside This is how the Depolarising Blockers act * Contraction requires a continuous entry of Na+ ions inside and subsequent release of Ca+ ions in the muscle -Textbook of Physiology by Guyton and Hall(2000),68,69
Similarly, if the muscle does not depolarise at all, it cannot contract*, and it remains relaxed + + + + + + + + Outside - - - - - - - - Inside This is how the Non-Depolarising Blockers act * Contraction requires a continuous entry of Na+ ions inside and subsequent release of Ca+ ions in the muscle -Textbook of Physiology by Guyton and Hall(2000),68,69
Thus,there are 2 types of NMBs Depolarising Act by Sustained Depolarisation and subsequent Blockade -Suxamethonium -Decamethonium Non-Depolarising Act by Competitive inhibition of Ach, hence called Competitive -Pancuronium -Vecuronium -Atracurium
Normal Depolarising NMBs Competitive NMBs Repolarisation Repolarisation Repolarisation Sustained Depolarisation and later block Competitive Antagonism of Ach A Ch acts = Depolarisation A Ch cannot act A Ch cannot act Plate repolarised Contraction Plate depolarised Relaxation Relaxation
General Anaesthesia Freedom from pain Neuro- Muscular Blocker Relaxation of skeletal muscles for operative ease Management of Bleeding IV set-up to access circulation Why are NMBs used in GA? Surgery requires
IV line is set up IV Thiopentone (GA) given which makes a patient unconscious IV NMB is given,which paralyses all skeletal muscles including tracheal and respiration stops!! Some initial steps in GA Preanaesthetic medication before patient is taken to the theatre
Intubation done and Ventilation continued (in place of respiration) throughout surgery After surgery, a reversal agent given which brings back respiration Some later steps in GA…... Now,the patient needs O2 urgently as he/she has stopped breathing
The Crucial Moments are between ‘Stoppage of Respiration’ and ‘Intubation’ Hence, onset of action of NMB must be as fast as possible, which would allow ‘Early Intubation’
Reversal Agent At the end of surgery,the effect of NMB must end.This is done by giving a reversal agent,antiChE which increases Ach at the NMJ. After a reversal agent is given, the recovery from NMB effect must be smooth and not erratic
Scene 1 Acetylcholine Cholinesterase
Scene 2 Acetylcholine Cholinesterase Rocuronium
Scene 3 Acetylcholine Cholinesterase CholinesteraseInhibitor Rocuronium