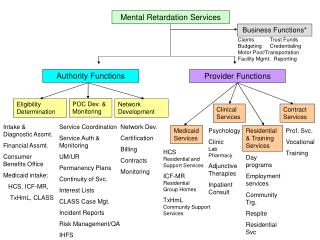
Mental Retardation
Mental Retardation. Dr. Y R Bhattarai TMU. terminology. amentia. Idiot , Imbecile. Mental retardation . Developmental delay. Developmental disabilities. What happens when the brain fails to mature and grow ? Child fail to develop and acquire milestones like normal children.

Mental Retardation
E N D
Presentation Transcript
Mental Retardation Dr. Y R Bhattarai TMU
terminology amentia Idiot, Imbecile Mental retardation Developmental delay
Developmental disabilities What happens when the brain fails to mature and grow ? • Child fail to develop and acquire milestones like normal children. • These conditions, in which there is a significant deficit or delay in the development of various mental functions from early childhood, are called developmental disabilities.
different types of developmental disabilities Mental retardation Autism Cerebral palsy Language developmental disorder Learning disability
Mental retardation Definition • condition in which there is delay or deficiency in all aspects of development, i.e. there is global and noticeable deficiency in the development of motor, cognitive, social, and language functions. • Mental retardation is a particular state of functioning that begins in childhood and characterized by limitation in both intelligence and adaptive skills. • Mental retardation is scored on axis II
Intelligence • refers to a general mental capability. • involves the ability to reason, plan, solve problems, think abstractly, comprehend complex ideas, learn quickly, and learn from experience. • scientific method of measuring intelligence is through standardized psychological tests called IQ tests. • Mental retardation is present if an individual has an IQ test score of approximately 70 or below.
Adaptive skills • refers to the skills needed to live independently. • Significant limitations in adaptive behavior impact a person’s daily life and affect the ability respond to a particular situation or to the environment. • Measured by standardized test
Types • daily living skills (practical), such as getting dressed, using the bathroom, and feeding oneself; • Communication (conceptual) skills, such as understanding what is said and being able to answer; money concepts • social skills with peers, family members, spouses, adults, others, understanding responsibility, following rules, being victims
diagnosis • Significant sub-average intellectual functioning • deficits in two or more Adaptive functioning • Onset before 18 years of age.
prevalence Mental retardation is a common condition. • India – 2% • Bangladesh - 2% • Thailand – 1.3% • USA – 1.6%-3%
Causes of MR Down syndrome, fetal alcohol syndrome and Fragile X syndrome are the three most common causes. Fetal accohol syndrome is the most common known cause Down and fragile X syndrome are most common genetic causes.
Downs Syndrome • accounts for 25-50% of persons with severe MR. • approximately 1 per 800 live births • extra chromosome 21 i.e, total 47 instead of 46 chromosomes
Fragile X syndrome • 1 in 3500 males • Results from mutation in X chromosome
Fetal alcohol syndrome • Entire syndrome occurs in around 15% of babies born to alcoholic mothers
INTELLIGENCE QUOTIENT(IQ) • Definition: a general estimate of the functional capacities of the person • 70% inherited, most from the mother • IQ is not an absolute score but a comparison among people. • Average IQ is between 90 to 109. • Calculating an IQ: (MA/CA)X 100= IQ score. • IQ is highly correlated with education and is an excellent predictor of academic achievements. • IQ is very stable from 5 yrs onward. • Increased exposure to verbal behavior early in life leads to higher IQ
COMMONLY USED IQ TESTS • Stanford- Binet scale is the first formal IQ test and is used for children aged 2 to 18. • Today it is the most useful with children younger than 6.
Class Mild MR-85% Moderate MR-10% Severe MR-4% Profound MR-1-2% IQ 50-69 35-49 20-34 < 20 Classification of MRaccording to IQ
Other features • Features of Syndrome • Prone to seizures • Additional psychiatric disorders • co morbidity seen in around 2/3rd patients • Disruptive disorder-mild MR • Self mutilating behaviors-severe MR • 2-3% -schizophrenia • 50%-mood disorders • ADHD symptoms • Repetitive stereotypic behaviors • Low self esteem, poor frustration tolerance • aggression
management • Primary prevention • Secondary prevention • Tertiary prevention
Primary prevention • Health education and awareness • Universal iodization, Universal immunization • Nutritional supplementation to pregnant ladies • Avoiding too early or too late pregnancy • spacing pregnancies • Avoiding exposure to harmful chemicals/drugs in prenatal, postnatal periods • Screening pregnant women for infections and promptly treating • Preventing Rh-isoimmunization • Providing stimulating environment • Amniocentesis • Genetic counseling
Secondary prevention • screening and dietary treatment for PKU • screening and thyroid hormone replacement therapy for congenital hypothyroidism
Tertiary prevention • Providing adaptive skills training, social skills training, vocational training • Providing job opportunities • Treating co-morbid medical and psychiatric illnesses
History • Word “autism” comes from Greek word “autos”- meaning self - coined by Swiss Psychiatrist Eugene • Earlier diagnosed as Childhood Psychosis
Leo Kanner, a Baltimore psychiatrist, termed early infantile autism / Kanner’ssyndrome
Definition Autism is a brain developmental disorder characterized by impaired social interaction and communication, and by restricted and repetitive behavior.
Prevalence • Prevalence is 2-5 per 10,000 live births. • Risk is 3-4 times higher in males than females • Onset is before age of 3 years
Characteristics • Social impairment • Communication impairment • Restricted repetitive behaviors • Others • Associated conditions
Social impairment • Infants -smile and look at others less often -respond less to their own name -no interest in social games • Toddlers -Have less eye contact, stay alone -Lack of peer relationships -Failure to use nonverbal social clues like body postures.
Children -have difficulty regulating their emotions -may show “immature” behavior such as crying in class or verbal outbursts that seem inappropriate • even be disruptive and physically aggressive at times, making social relationships more difficult
“lose control,” particularly when they're in a strange or overwhelming environment, or when angry and frustrated, at times break things, attack others, or hurt themselves, in their frustration, some bang their heads, pull their hair, or bite their arms. -For older children making and maintaining friendships often proves to be difficult
Communication impairment • About 40% of children with Autism do not talk at all. • Another 25%–30% of children with autism have some words at 12 to 18 months of age and then lose them. • Others may speak, but not until later in childhood.
unable to combine words into meaningful sentences • Some speak only single words, while others repeat the same phrase over and over. Some repeat what they hear (echolalia) • have great difficulty in sustaining a conversation • have a hard time using and understanding gestures, body language, or tone of voice. • Facial expressions, movements, and gestures may not match what they are saying.
voices might sound flat or high-pitched. • might stick with one topic of conversation for too long • less likely to make requests or share experiences • Pronoun reversals – eg. “you want the toy” for I want it.
Restricted repetitive behavior • self-stimulation behaviors - repeatedly flapping their arms or rocking from side to side • repeatedly turn a light on and off or spin the wheels of a toy car in front of their eyes • Self injurious behavior-skin picking, hand biting, head banging
RESTRICTED BEHAVIOR • An inflexible adherence to specific non functional routines or rituals e.g. eating the same meal in the same manner in the same place at the same time of the day. • Arrange objects in certain way • Persistent preoccupation with the parts of objects e.g. buttons • Repetitive motor mannerisms e.g. whole-body rocking
Others • Unusual responses to sensory stimuli - under-responsivity (for e.g. walking into things) -over-responsivity (for e.g. distress from loud noises) • Associated motor problems – poor muscle tone • Unusual eating behaviors • Sleep problems • Minor physical anomalies
Associated disorders • 25%-75% - mental retardation • 1/4 – epilepsy • 1-5% - Fragile X syndrome • 1-4% - Tuberous sclerosis • Anxiety and Depression • Learning disabilities
Causes • The cause is CNS damage due to known or unknown factors • Genetic factors -Often familial, 2-4% siblings might be affected -Rare mutations • Environmental factors -Perinatal birth complications -Teratogens – heavy metals, pesticides, alcohol, smoking -infections like encephalitis, maternal rubella, PKU etc.
Management The main goals of treatment are • to lessen associated deficits and family distress • to increase quality of life and functional independence
Special education programme • Behavior therapy • Family counseling • Medications (newer antipsychotics) for co- morbid disorders • Anxiety, depression • Seizures • Self injurious behavior
Prognosis • Lifelong disorder • Based on adult study outcome • 2/3rd – dependent • 1-2% - independent • 5-20% - boderline normal status