### Understanding the Uninsured: Health Impacts and Economic Challenges ###
1.56k likes | 1.7k Vues
This report examines the challenges faced by uninsured individuals, including statistics on health impacts, bankruptcies related to medical costs, and disparities in access to care. It highlights the demographics of the uninsured, such as students, homemakers, and the disabled, and reveals that many with insurance have limited choices. The findings illustrate the significant financial burden of healthcare, with a high percentage of bankruptcies linked to medical debts. Additionally, the report discusses the implications of managed care on patient outcomes and the urgent need for reform in the healthcare system to ensure equitable access. ###

### Understanding the Uninsured: Health Impacts and Economic Challenges ###
E N D
Presentation Transcript
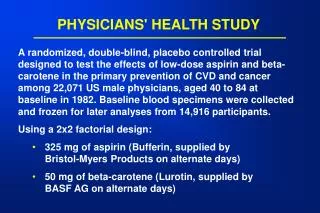
PHYSICIANS FOR A NATIONAL HEALTH PROGRAM 29 EAST MADISONSUITE 602CHICAGO, IL 60602TEL: (312) 782-6006WWW.PNHP.ORG
Who Are The Uninsured? *Students>18, Homemakers, Disabled, Early retirees Source: Himmelstein & Woolhandler - Tabulation from 1999 CPS
Full Time Jobs Provide LittleProtection for Hispanics Source: Commonwealth Fund, 3/2000
Rising Out-of-Pocket Costs for SeniorsVoucher/Premium Support Proposals Would Worsen Percent of Income Source: Senate Select Committee on Aging; AARP 4/95 & 3/98; and Commonwealth Fund May, 1999 projections (adjusted to include nursing home costs)
Who Pays for Nursing Home Care? Source: Health Affairs 2000; 19(3):44
Illness and Medical Costs,A Major Cause of Bankruptcy • 45.6% of all bankruptcies involve a medical reason or large medical debt • 326,441 families identified illness/injury as the main reason for bankruptcy in 1999 • An additional 269,757 had large medical debts at time of bankruptcy • 7 per 1000 single women, and 5 per 1000 men suffered medical-related bankruptcy in 1999 Source: Norton's Bankruptcy Advisor, May, 2000
Many With Insurance Lack Choice42% Are Offered Only 1 Plan Note: Those without choice were 70% more likely to give their plan a low rating Source: Health Affairs 1998; 17(5):184
Patients Refused Authorization for ER Care • 8% to 12% of HMO patients presenting to 2 ERs were denied authorization • Authorization delayed care by 20 to 150 minutes • Of those denied: 47% had unstable vital signs or other high risk indicators 40% of children were not seen in f/u by primary MD Eventual diagnoses included: meningococcemia (2), ruptured ectopic (2),shock due to hemorrhage (2), septic hip, PE, MI (2), ruptured AAA, pancreatitis, peritonsillar abscess, small bowel obstruction, unstable angina, pneumothorax, appendicitis, meningitis(3) Source: J Emerg Med 1997; 15:605; Acad Emerg Med 1997; 4:1129; Ann Emerg med 1990; 19:59
Financial Suffering at the End of Life Source: Ann Int Med 2000; 132:451 - Study of 988 terminally ill patients* Out-of-pocket medical costs > 10% of household income** Patient or family sold assets, took out mortgage, used savings or took extra job
Why Women Delay Prenatal CareWhen They Know They Are Pregnant Note: 11.1% of pregnant women failed to get timely prenatal care despite knowing they were pregnant Source: MMWR 5/12/2000; 49:393
Poverty Rates, 1997U.S. and Other Industrialized Nations Source: Luxembourg Income Study Working PapersNote: U.S. figure for 1997, other nations most recent available year
Americans Lead the World in Hours Worked Source: International Labor Organization, 1999
Causes Of Excess Deaths AmongAfrican Americans Cardiovascular 39% Cardiovascular 25% Source: Himmelstein & Woolhandler - Analysis of data from NCHS
Pharmacies in Minority NeighborhoodsFail to Stock Opioids Source: N Engl J Med 2000; 242:1023
Minority Physicians ProvideMore Care for the Disadvantaged Ethnicity of Physician Source: AJPH 1997;87:817
Are Emily and Brendan More Employable than Lakisha and Jamal?
Growth of Registered Nurses and Administrators1970-2002 Source: Bureau of Labor Statistics & Himmelstein/Woolhandler/Lewontin Analysis of CPS data
Growth of Physicians and Administrators1970-2002 Source: Bureau of Labor Statistics & NCHS
High Risk HMO Patients FaredPoorly in the Rand Experiment Source: Rand Health Insurance Experiment, Lancet 1986; i:1017Note: High Risk = 20% of population with lowest income + highest medical risk
The Elderly and Sick Poor did Worse in HMOs Changes in Physical Health at 4 Years Source: Medical Outcomes Study - JAMA 1996;276:1039
Elderly HMO Stroke PatientsGet Less Specialist Neurology Care Source: Medical Care 1999; 37:1186Note: Patients receiving specialist neurology care had 23% lower 1 year mortality
HMOs' Stroke Patients:Fewer Go Home or to Rehab, More to Nursing Homes Source: JAMA 1997; 278:119
HMOs Push Heart Surgery Patientsto High-Mortality Hospitals Source: JAMA 2000; 283:1976*CABG = coronary artery bypass graft surgery
Fee-For-Service Managed Care Primary Care Patients Depression Detected 53.7% 41.8% Appropriately Treated 60.7% 46.4% Patients Seeing Psychiatrist # Functional Limitations - Baseline 1.3 1.5 # Functional Limitations - 2 Years 1.2 2.0 Depressed Patients:Fee-for Service Vs. Managed Care SOURCE: Medical Outcomes Study - JAMA 1989;262:3298 & Arch Gen Psych 1993; 50:517
Managed Mental Health: Audit Report • Plans overstated utilization by 45% • Delay from initial call to starting care > contractor's written standard by 97%-347% • Plans rarely site-visited or interviewed providers • No providers in 15% of counties "covered"; no child provider in 25% of counties • Quality problem in 30-58% of charts reviewed • Criteria for inpatient care dangerously restrictive (eg. requiring DTs prior to detox admit) • Overhead + profit NEVER consumed < 45% of premiums Source: J. Wrich - Audit findings submitted to CBO, 3/98
Primary Care Physicians: Patients Can't Get Quality Mental Health Services Source: Center for Studying Health System Change, 1997 - survey of 5,160 primary care physicians Note - Data shown are for inpatient care; responses regarding outpatient care were similar
States that Limit New Heart Surgery Programs: Higher Volumes, Lower Mortality
Can Seniors Make Informed HMO Choices?Proportion with Knowledge of How HMOs Work Source: AARP Survey - Health Affairs 1998; 17(6):181