Download
1 / 31
310 likes | 574 Vues
Global Health: the Zimbabwe and Haiti Cholera Epidemics. J. Glenn Morris, Jr., MD, MPH&TM UF Emerging Pathogens Institute. 900. Unintentional injury. Group III - Injuries. Intentional injury. 800. Other non-communicable. 700. Neuro-psychiatric. Group II - Noncommunicable conditions.

E N D
Global Health:the Zimbabwe and Haiti Cholera Epidemics J. Glenn Morris, Jr., MD, MPH&TM UF Emerging Pathogens Institute
900 Unintentional injury Group III - Injuries Intentional injury 800 Other non-communicable 700 Neuro-psychiatric Group II - Noncommunicable conditions 600 Chronic respiratory 500 Cancer DALYs (000,000s) Vascular 400 Group 1 - Communicable diseases, maternal and perinatal conditions and nutritional deficiencies Nutritional 300 Maternal and perinatal 200 Respiratory infections Infectious and parasitic diseases 100 0 Developing –high mortality Developing –lower mortality Developed Amount and patterns of disease burden in 3 major world regions Population 2.3 2.4 1.3 (billions)
Global distribution of mortality attributable to 20 leading selected risk factors High blood pressure Tobacco High cholesterol Underweight Unsafe sex Low fruit and vegetables High BMI Physical inactivity Alcohol Unsafe water, S&H Indoor smoke from solid fuels Developing high mortality Developing lower mortality Iron deficiency Developed Urban air pollution Zinc deficiency Vitamin A deficiency Unsafe health care injections Occupational particulates Occupational injury Lead exposure Illicit drugs 0 1 2 3 4 5 6 7 8 Attributable mortality in millions (Total 55.9 million)
Global Health • Issues that impact global health • Increasing income differentials among countries that foster poverty-associated conditions for poor health • Variance in environmental and occupational health and safety standards that contribute to dangerous working conditions • Global environmental change leading to such things as depletion of freshwater supplies and the loss of arable lands • Re-emergence of infectious diseases • Defining the role of the Developed World • Easterly: “The White Man’s Burden”
The Critical Importance of Sustainability Give a man a fish and you feed him for a day. Teach a man to fish and you feed him for a lifetime. Chinese Proverb
Lunchtime Global Health Talks(Courtesy of the Hispanic American Medical Student Association [HAMSA], the Emerging Pathogens Institute, and the Department of Environmental and Global Health, PHHP) • January 4, Dr. Glenn Morris • Global Health: the Zimbabwe and Haiti Cholera Epidemics • February 8, Dr. Mike Lauzardo • Mexico – Our most important partner in global health • March 29, Dr. Charles Hobson • April 19, Dr. Greg Gray • Opportunities for health professionals in global health
Cholera and Cholera Toxin • Action • Constitutive activation of adenylate cyclase by A1 subunit, through G protein, probably for life of cell • Results in increased intracellular cAMP concentrations, leading to increased Cl- secretion by intestinal crypt cells and decreased NaCl coupled absorption by villus cells • Net movement of electrolytes results in water flow into the lumen of the intestine • Does NOT affect glucose-mediated transport
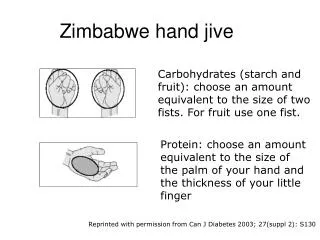
“The discovery that sodium transport and glucose transport are coupled in the small intestine, so that glucose accelerates absorption of solute and water, was potentially the most important medical advance this century.” Lancet, 1978
Environmental Parameters V. cholerae in environment including plankton Cholera infections in humans Cholera Transmission Pathways Spatio-Temporal Heterogeneity
Why did the Zimbabwe Epidemic Occur? • Major driver: breakdown of public health infrastructure/water and sewerage systems • Other factors? • Pattern of spatial spread • Contribution of human direct vs. environmental transmission • Potential impact of vaccination
Map of Zimbabwe, provinces and neighboring countries. The red colored regions show one of the cholera affected districts (Manica) in Mozambique in 2006 and some of the cholera affected provinces (Southern and Lusaka) in Zambia in 2010 which are on the border with Zimbabwe.
Zimbabwe • Spatial Models • SIR model • Calculation of R0 • Average number of secondary infections that occur when one infective is introduced into a completely susceptible host population • Estimation of relative contributions of: • human/human transmission (short cycle, increased infectivity) vs. • human/environment/human (long cycle, decreased infectivity) • Use of these estimates to assess utility of intervention strategies
Case Clusters, Weeks 1-5 First cases: Karibe district (on border with Zambia): peak weeks 1-2 Major initial epidemics: Beitbridge (on South African border): peak weeks 2-3 Harare (capital): peak weeks 4-5 Spread to district centers ? Importance of funeral celebrations
Relative Contribution of “Human” vs. “Environmental” Source • Zimbabwe • RE (long cycle) = 0.20 (95% CI: 0.15-0.2); 17% • RH (short cycle) = 0.95 (95% CI: 0.93-0.98); 83% • R0 = 1.15 (95% CI: 1.08-1.23)
Summary - Zimbabwe • Stepwise spread of illness from key urban centers into districts • R0 varied by province, indicative of differences in transmission dynamics • Values of R0 were in range of 1.11-2.72 • Major contribution from human/human (short cycle) transmission – but both modes of transmission necessary to maintain epidemic • While there was wide variation in needed vaccination coverage, based on R0, data provide insight into how transmission could be stopped Key contribution: Understanding of transmission dynamics, and approaches to vaccine use, that can guide interventions of Ministry of Health
Haiti: Earthquake, January 12, 2010 Almost total destruction of public health infrastructure, including water and sewerage
PHHP/IFAS: Long-term Focus on Development of Sustainable Community
Cholera: October 21, 2010 • While destruction of public health infrastructure made Haiti “high risk” for cholera, no cases present in the country since 1960 • First cases – along Artibonite River • Association of cases with river • PFGE – isolates clonal • UN unit from Nepal at epicenter of outbreak • Rapid subsequent spread throughout country
UF Involvement in Cholera Outbreak • Focus on sustainability, data collection to guide subsequent interventions • Oral rehydration • Preparation of 2,000 ORS packets by Pharmacy students • Distribution of >1,000 copies of instructions for ORS in Creole • Outbreak assessment • Assessment of clonality • Application of mathematical models
VNTR loci vary by the number of repeated units Repeating unit is the hexamer AACAGC
Distribution of Vibrio cholerae VNTR sequence types among 190 V. cholerae isolates from 13 Haitian patients with severe diarrhea. Numbers represent number of repeats for the four alleles tested: VC0147, VC0437, VC1650, and VCA0171, respectively. A is the dominant sequence type, identified in 12 of 13 patients for whom VNTR data were available; B, C, and D were each present in one patient, with patients having type B or type C also having type A.
Haiti Estimates: 10/31-11/29/2010 Ouest includes Ouest** and Port-au-Prince
Summary - Haiti • Outbreak from apparent common source, with rapid spread facilitated by total destruction of public health infrastructure • R0 varied by province, indicative of differences in transmission dynamics • Values of R0 were in range of 1.1-2.03 • Effective vaccination coverage would require immunization of 10-56% of population in various provinces Key contributions • Immediate provision of ORS, with concurrent education program • Understanding of transmission dynamics, and approaches to vaccine use, that can guide interventions of Ministry of Health
How do you do “Sustainability”? • Provide means of facilitating long-term local efforts to control disease • Research • Understanding of disease transmission pathways, new vaccines, new drugs for neglected diseases • Education • Assist with development of sustainable public health infrastructure • Water and sewerage systems • Nutrition programs • Vaccination programs • General education programs