Duke Case Review
Duke Case Review. Patient’s History. HPI: 52 year old woman presents with two weeks of diplopia and headache. Physical exam: Left partial sixth nerve palsy. Reports diplopia on bilateral lateral gaze. What is true about this vascular anomaly?. 1) There is a single, large basilar aneurysm

Duke Case Review
E N D
Presentation Transcript
Patient’s History • HPI: 52 year old woman presents with two weeks of diplopia and headache. • Physical exam: Left partial sixth nerve palsy. Reports diplopia on bilateral lateral gaze.
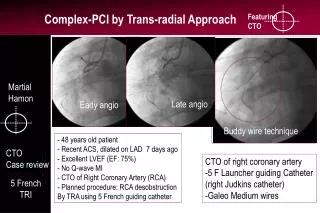
What is true about this vascular anomaly? • 1) There is a single, large basilar aneurysm • 2) The aneurysm has a narrow neck • 3) The basilar artery is fenestrated • 4) There is no thrombus within the aneurysm.
Smaller Aneurysm Wide Aneurysm Neck Fenestrated Basilar Artery
What is true? • 1) The 5 year rupture rate of a 5 mm aneurysm is 5 % • 2) The 5 year rupture rate of a 25 mm basilar aneurysm is 50% • 3) Narrow neck aneurysms are more difficult to treat • 4) Basilar aneurysms are easier to clip • 5) MCA aneurysms are easier to coil than clip.
Corrected answers • 1) The 5 year rupture rate of a 5 mm aneurysm is .01 % • 2) The 5 year rupture rate of a 25 mm basilar aneurysm is 50% • 3) Narrow neck aneurysms are easier to treat • 4) Basilar aneurysms are easier to coil • 5) MCA aneurysms are easier to clip
Findings • Giant, broad-necked basilar aneurysm measuring 26 mm in greatest dimension. • How do you treat this aneurysm? • Does the fenestration affect your treatment plan? • What are you going to do about the smaller 3 mm aneurysm?
Which of the following risks of the procedure is the most likely to occur? • 1) Aneurysm swelling post-coiling requiring steroids to prevent symptoms. • 2) Embolic stroke. • 3) Coil compaction requiring repeat procedure. • 4) Aneurysm rupture due to manipulation of the aneurysm.
Which of the following risks of the procedure is the most likely to occur? • 1) Aneurysm swelling post-coiling requiring steroids to prevent symptoms. • 2) Embolic stroke. • 3) Coil compaction requiring repeat procedure. • 4) Aneurysm rupture due to manipulation of the aneurysm.
Which of the following risks of the procedure is the most likely to occur? • 1) Aneurysm swelling post-coiling requiring steroids to prevent symptoms. • 2) Embolic stroke. • 3) Coil compaction requiring repeat procedure. • 4) Aneurysm rupture due to manipulation of the aneurysm.
Conclusion • 1) Rupture rate for aneurysms < 7mm is low (.01% per year) and, if they are asymptomatic, most would recommend serial imaging rather than therapy. • 2) The location, size and neck of the aneurysm are all important factors when planning therapy. • 3) Coiling is generally favored over clipping of aneurysms. • 4) Use the neuroform stent for broad necked aneurysms.