PCOS
PCOS. Chairman of the Indian College of Obstetricians & Gynecologists (ICOG) Past President of the Federation of Obstetric & Gynecological Societies of India (FOGSI) 2006 Honorary Fellow of the Royal College of Obstetricians & Gynecologists

PCOS
E N D
Presentation Transcript
Chairman of the Indian College of Obstetricians & Gynecologists (ICOG) • Past President of the Federation of Obstetric & Gynecological Societies of India (FOGSI) 2006 • Honorary Fellow of the Royal College of Obstetricians & Gynecologists • Prof. and Cons. Obs. & Gyn,Breach Candy Hospital, Jaslok Hospital, Sir H.N. Hospital Mumbai, India.
1999 Criteria (all) NIH/NICHD oligoovulation Clinical and / or biochemical signs of hyperandrogenism exclusion of other etiologies. 2003 Criteria (2 out of 3) ESHRE/ASRM Oligo and / or anovulation Clinical and / or biochemical signs of hyperandrogenism. Polycystic ovaries US exclusion of other etiologies PCOS – Definition Gynaecworld Contd…..
Clinical signs of androgen excess Hirsutism Acne Biochemical signs of androgen excess ↑ Androstenedione ↑ Free testosterone ↑ DHEAS ↑ Free androgen index ↑ LH levels PCOS – Definition Gynaecworld Contd…..
Other Etiologies. Congenital adrenal hyperplasia Androgen secreting tumors Cushings syndrome Thyroid dysfunction Hyper prolactinemia Drug induced Androgen excess PCOS – Definition
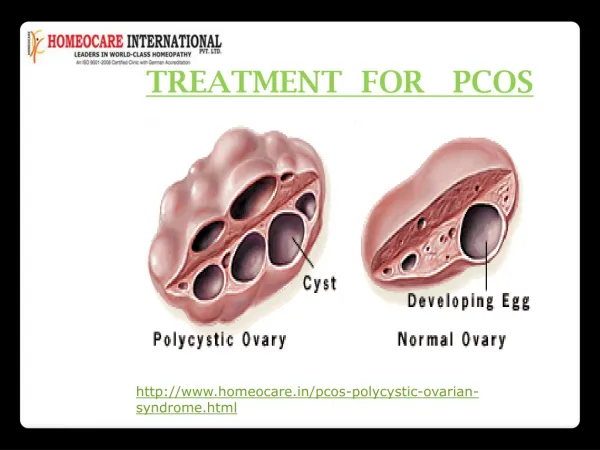
Ultrasound ∆ of PCOS ROTTERDAM CRITERIA In one or both ovaries • ovarian volume > 10 ml • ≥ 12 follicles, 2-9mm in diameter • Echo dense stroma
Origin and sequelae of abnormal neuroendocrin function in PCOS PCOS Women Persistent rapid LH dysfunction (1LH pulse/hour) ↑ LH & LH : FSH ratio ↓ FSH ↑ ovarian androgens Impaired follicular development Impaired hypothalamic Progesterone sensitivity Impaired Progesterone production Source : Blank SK et al Hum Reprod updare 2006 Jul - Aug
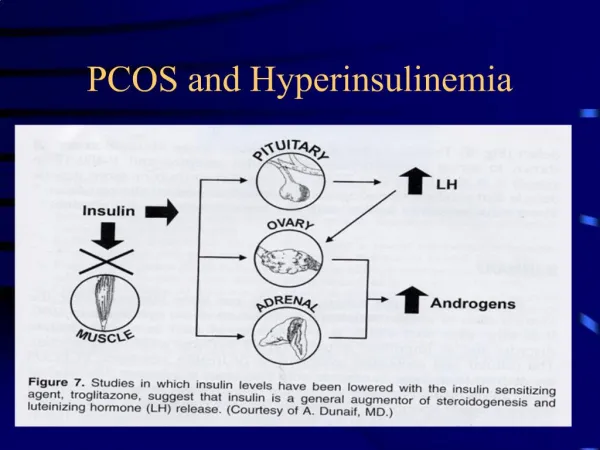
Hyperinsulinaemia & Hyperandrogenaemia Insulin Receptor Dysfunction Hypothalamus LHRH Pancreas Pituitary Hyperinsulinaemia LH FSH Liver Adrenal Stroma Follicle Elevated DHEAS Reduced SHBG Elevated Androgens áFree androgens
Hyperandrogenism DHEA, DHEAS Androstenedione Testosterone ( Principal circulating androgen) ( Weak androgens metabolized in skin ) Dihydrotestosterone ( DHT ) Potent androgens Dermal papilla Vellus hair Terminal medulated hair
Clinical Presentation of Women with PCOS Reproductive Period Menopausal Adolescent Period • Menstrual • Irregularity • Cosmetic concerns • Acne • Hirsutism • Hair Loss • Infertility • Early Pregnancy loss • During pregnancy • PIH • GDM • Metabolic • Syndrome • Ca Endometrium Obesity
Diet • Low in saturated fats - ↑ in dietary fiber - low glycemic – index • carbohydrates • Low glycemic index foods • include bran, cereals, mixed • grain breads, lentils and soya Ref : Kathleen Metal Clin Obst Gynecol 2007
Exercise • American Diabetes Association recommends minimum of :- • 150 minutes/week of moderate to vigorous exercise • for individuals with IGT. • Should be distributed over 3 days • For long term weight reduction – 1 hour/day of • exercise is recommended. Ref : Kathleen Metal Clin Obst Gynecol 2007
Role of weight loss • Conclusions: • Weight loss plays a significant role in restoration of ovulation in obese women with PCOS Ref : Kathleen M et al Fertility & Sterility 2004
Why does PCOS lead to infertility? Ovulation Poor Oocyte Quality Fertilization Endometrial Abnormality Implantation Effects Hyperinsulinemia Fetal Viability ?Effects gestational Diabetes and hypertension Healthy Live born Ref : Hum Reprod 2004: 19
Infertility to Fertility- Management overview Specific programs For lifestyle Modifications (atleast 6 months) in Obese women BMI Clomiphene Citrate LOD (in infertile PCOS pts when co-factors of sub fertility are suspected and/or diagnosed) Metformin Gonadotropins Metformin+CC COS+TI / IUI ARTs Metformin+ Gonadotropins (?) PREGNANCY Palomba. Ovulation induction in PCOS. Fertil Steril 2006
Consensus in Management of PCOS related to Infertility • No consensus in management before 2007 • In March 2007 at Thessaloniki Greece, The Thessaloniki ESHRE/ASRM- Sponsored PCOS Consensus Workshop Group reached a consensus in management of PCOS related to infertility and made few conclusions. - Published in Fertility Sterility 2008
Conclusions of The Thessaloniki ESHRE/ ASRM- Sponsored PCOS Consensus Workshop Group -2007
Before any intervention is initiated, preconception counselling should be provided Emphasis on: • Diet – Hypocaloric diet • Exercise – long term, aim to reduce 5-10% body weight • Avoiding Alcohol & smoking Cont…….
The recommended first–line treatmentfor OI is CC. • Recommended second-linein CC resistance isGonadotropins with or without IUI or LOS. • Both have distinct advantages and drawbacks Cont…….
Choice should be made on an individual basis. Use of Gonadotropins • multiple pregnancy • intense monitoring LOS effective in <50% of women • additional ovulation induction is required under those circumstances. Cont…….
Recommended third-line treatment is IVF, because this treatment is effective in women with PCOS undergoing IVF. Single ET reduces chances of multiple pregnancy. Cont…….
Metformin use in PCOS should be restricted to women with glucose intolerance. Based on recent data available in the literature, the routine use of this drug in ovulation induction is not recommended. Cont…….
Insufficient evidence is currently available to recommend the clinical use of aromatase inhibitors for routine ovulation induction.
PCOS and ART Offered to Women • Who fail to conceive after 6 cycles of Ovulation Induction • As an alternative to women in whom OHSS appears imminent • Who have repeated cycles of LUF
PCOS & ART Factors affecting results: • Ovarian volume • Antral Follicles • Ovulation Induction Protocols • Oocyte Retrieval • Occurrence of OHSS • Luteal Support
Pathogenesis of early pregnancy loss in PCOS Hyper secretion of LH Hyperandrogenaemia Hyperinsulinemia Obesity ▪ Plasminogen activator inhibitor activity ▪ endothelial dysfunction Disordered ovarian and endometrial function Early Pregnancy loss WOMEN WITH PCOS HAVE AN PREVALENCE OF MISCARRIAGE, BOTH AFTER SPONTANEOUS & INDUCED OVULATION Ref : Vander spuy ZM et al Best pract Res clin Obstet Gynaecol 2006 Oct.
Preterm birth 1.75 (1.16-2.62) Role of PIH 3,67 (1,98-6.81) Risk of GDM 2.94 (1.70-5.08) Risk of NICU adm. 2.31 (1.25-4.26) 3.07 (1.03-9.21) PCOS Non-PCOS Pregnancy outcomes in women with PCOS • Meta analysis: • 15 studies • 720 women with PCOS • 4505 controls Risk of perinatal mortality Conclusion: Women with PCOS are at increased risk of pregnancy and neonatal complications Ref : CM et al Hum Reprod Update 2006
Metformin use during pregnancy • Meta-analysis of 8 studies on pregnancy outcome → no risk of major malformations • Few Observational studies have suggested a lower risk of GDM & PIH in users Cont…
Metformin use during pregnancy Study on Neonates :- Evaluation of 126 infants born to 109 pcos mothers who continued metformin through out pregnancy. Conclusions:- • Metformin reduces GDM • Not Teratogenic • No effect on BW, Growth or Motorsocial development in first 18 months of life. Hellmuth et al, Diabet Med 2000, 17:507-511
Insulin Resistance: Associated Conditions Type 2 diabetes Atherosclerosis Hypertension Dyslipidemia Insulin Resistance Impaired Glucose tolerance Decreased Fibrinolytic Activity Obesity (central) Acanthosis Nigricans Polycystic ovary disease Hyperuricemia
PCOS & Metabolic Syndrome Metabolic Syndrome: • Cluster of Cardiovascular risk factors related to Insulin Resistance:- Obesity- Hyperinsulinemia- Hypertension- Atherogenic Dyslipidemia- Atherosclerosis- Hyperglycemia • Major Risk Factors:- Physical inactivity- Atherogenic diet- Adiposity / abdominal obesity
Criteria for Metabolic Syndrome in PCOS • Abdominal Obesity (waist circumference >88 cm) • Triglycerides > 150 mg/100 ml • HDL Cholesterol <50 mg/100 ml • BP Systolic > 130 mmHgDiastolic > 85 mmHg • FBS > 110 mg % If any 3 of the 5 are present Metabolic Syndrome Ref: Zeyneloglu HB et al; Polycystic Ovary Syndrome Kent UK: Anshan Publishers 2006:102-112
PCOS & Diabetes • High prevalence of Type 2 Diabetes reaching epidemic levels in Asia • Insulin Resistance is often the precursor of Diabetes • Significantly prevalence of:- Obesity- Hypertension- triglycerides- LDL Liporotein- HDLin Asian Indians with IRS Ref: Yoon KH et al Lancet 2006; 368:1681-1688Deedwania PC et al J Assoc Physicians India 2006;54:797-810Gupta A et al Diabetes Res Clin Prac 2003;61:69-76
PCOS & Obesity • Obesity linked to risk of Type II Diabetes- 30% of obese PCOS women have ) by the impaired GTT ) age of 40 - 7.5% have frank Diabetes ) years • Obesity contributes significantly to - both IR & HA in women with & without PCOS- menstrual disorders- worsens clinical presentation Ref: Park KH et al; Int J Gynecol Obstet 2001; 74: 261-267 EK I et al; J Clin Endocrinol Metab 1997; 82:1147-1153 Contd..
Central Obesity IDF: Central obesity - Waist circumference >94 cm in men, >80 cm in women with ethnicity specific values for other groups WHO: - Waist-hip ratio >0.9 - men >0.85 - women ATP III: Waist circumference >40 in. - men, > 35 in. - women
Prevalence of Hirsutism • 1.2 to 18% of women in reproductive age group • PCOS responsible for 60-90% of hirsutism • CAH responsible for 2 to 5% • 20% Idiopathic Nikolan; Curr Obst & Gyn (2005) 15, 174-182Azziz R, Endocrine Reviews 21(4): 347-362 Ferriman & Gallwey, 1961, J of Clinical Endocrinology Contd..
Scoring Hirsutism: Modified Ferriman Gallway Score • Ferriman Gallway was modified since hair growth over forearm and lower leg was less sensitive or indifferent to androgens • 9 sites • Scored 0 to 4 • Max score of 36 • Terminal hair defined as coarse pigmented medullated hairs, generally growing > 1 cm in length if uncut Contd..
Principles of treatment of hirsutism • Best results are achieved by combination treatment, including antiandrogens, suppression and topical treatments • Goal of medical therapy should be to reduce the time spent mechanically removing unwanted hair. • Most antiandrogens have similar efficacy. The choice of drug depends mainly on its tolerability by each individual patient.
Hirsutism Management Mechanical or Cosmetic Therapy • Shaving • Bleaching • Electrolysis • Laser Hormonal Therapy • Ovarian androgen suppression • Oral contraceptives • High dose progestin Adrenal Androgen Suppression • Dexamethasone • Thermolysis • Depilitation • Plucking • Long acting GnRh analogs • High dose estrogen
Drospirenone in PCOS CLINICAL BENEFITS • Helpful in treatment of Hirsutism • Excellent cycle control • Decreases acne • No weight gain. METABOLIC BENEFITS • No effect on carbohydrate metabolism • No deterioration in the glycemic and insulinemic response to glucose load. • No effect on serum lipid concentration. • Safe for long term use Gynaecworld
Current Strategies for PCOS In vitro maturation of oocytes Early follicular aspiration in hyper responsive pts. during ART Sequential stimulation protocol for ovulationinduction Reducing the dose of HCG to 2.500 IU fortrigger Initiating GnRh Antagonist on Day 1 ofstimulation Contd …..