Download
1 / 23
230 likes | 654 Vues
Coverage of Thigh. Ian Maxwell. Gastocnemius Flap. Mathes and Nahai type I muscle flap Indications Most commonly upper third of leg defects and knee Exposed bone, tendon, metal Can be advanced on its pedicle as a V-Y for achilles coverage Can be used as a functional muscle free flap

E N D
Coverage of Thigh Ian Maxwell
Gastocnemius Flap • Mathes and Nahai type I muscle flap • Indications • Most commonly upper third of leg defects and knee • Exposed bone, tendon, metal • Can be advanced on its pedicle as a V-Y for achilles coverage • Can be used as a functional muscle free flap • Lateral or medial heads can be taken
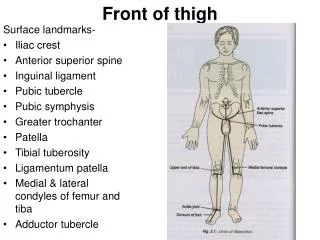
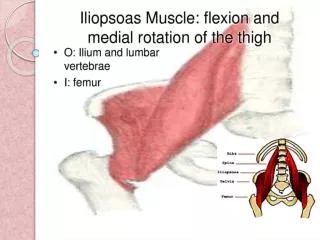
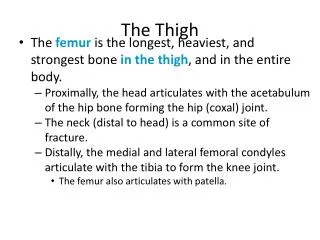
Muscle Anatomy • Origin: • Lateral head: Lateral epicondyle of femur • Medial head: Superior to medial epicondyle • Posterior to insertion of adductor magnus • Insertion • Calcaneal epiphysis via achilles tendon
Vascular Anatomy • Medial head: Medial sural artery from popliteal artery (1cm proximal to knee joint) • 4-5cm from origin of artery to muscle insertion • Lateral head: Lateral Sural artery • Pedicle length of 4cm (arises more distally) • Venous drainage via venae comitantes
Innervation • Tibial nerve
Flap dissection • Midcalf longitudinal or straight incision beginning a few centimeters proximal to popliteal crease • Sural vein and saphenous nerve retracted laterally • Medial and lateral heads dissected in popliteal fossa and continued distally to achilles tendon
Flap dissection • Medial head is cut from Achilles tendon • Dissect through loose areolar plane proximally between soleus and medial head of gastroc • Dissect pedicle • If necessary proximally divide origin • Tunnel subcutaneously to defect
Lateral head • More difficult • Common peroneal nerve at increased risk • Shorter pedicle length • Sometimes necessary of medial head flap can’t reach defect
Anterolateral thigh Flap • A type B and C (septocutaneous and musculocutaneous perforators) fasciocutaneous flap • Useful for local or distant defect reconstruction • Flap size up to 8cm X 25cm with primary closure • Indications: • Free: anywhere • Local: Thin flap, large surface area wounds • Groin, knee, abdomen, trochanteric region
Arterial Supply • Lateral femoral circumflex artery • Arises from lateral side of profundafemoris • Runs obliquely in septum between vastislateralis and rectus femoris • Pedicle length is 12-16 cm • For retrograde, distally based flaps can base it off of the lateral superior geniculate artery
Venous drainage • From venae comitantes accompanying artery
Innervation • Lateral femoral cutaneous nerve of thigh • Can harvest as a sensate flap
Flap elevation • Mark ASIS and lateral patella • This is the central axis of the flap • Draw a circle of radius 3cm in the middle of the line • This is where the perforators are • Doppler them • Base your flap around these perforators
Flap dissection • Dissect anteriorly first down to deep fascia • Dissect subfascial anterior to posterior • Vessels near or approaching the septum are preserved • Dissect posterior to anterior
Flap dissection • If vessels are perforators are all septocutaneous then elevate on these • If musculocutaeous then these must be dissescted out • Follow pedicle proximally and ligate if free or preserve if pedicled • If bulk is needed can preserve branches to VL or RF and take muscle with the flap
References • Microsurgeon.org • Serafin, d. Atlas of microsurgical tissue transplantation • Wei, Mardini. Flaps and reconstructive surgery