Download
1 / 60
600 likes | 690 Vues
Explore the physiology of the autonomic nervous system, its origins, functions, and relationships between sympathetic and parasympathetic divisions. Learn about autonomic ganglia and their types, sympathetic distribution, and effects on different organ systems.

E N D
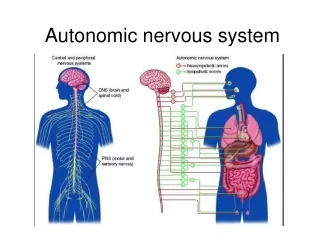
AUTONOMIC NRVOUS SYSTEM Definition:It is the system for involuntary subconscious functions , it controls the internal environment to maintain homeostasis . DIVISION OF NERVOUS SYSTEM : 1- Central nervous system : a) Brain b) Spinal cord 2- Peripheral nervous system : a) Cranial nerves Autonomic (involuntary) Somatic (voluntary) b) Spinal nerves Autonomic Somatic
A.N.S differs from Somatic N.S in :-In A.N.S there is : 1-Autonomic ganglia 2-Connector neurone is outside CNS 3-It regulates smooth muscles Q: Discuss and differentiate the two divisions of A.N.S ?
A.N.SSympatheticParasympathetic 1- ORIGIN: Thoraco-Lumber Cranio - sacral(Tl - T12 , LI,2,3) 3,7,9,10 S2 , 3 , 4 1- ORIGIN: Thoraco-Lumber Cranio - sacral(Tl - T12 , LI,2,3) 3,7,9,10, s2,3,4, 2-FUNCTION: Stress muscular exercise - Digestion and sleep, fear Empting fightmicturationflightdefication - Catabolic - Anabolic (energy lost from the body)(energy preserved) 4- DISTRIBUTION: widspreadLocalised 5- DISCHARGE : as one unit (most actions) To each system at the same time) separetly
RELATIONSHIP BETWEEN SYMP ATHETC AND PARASYMPATHETIC 1- RECIPROCAL : once sympathetic is stimulated, parasympaethetic is inhibited and vise - versa 2- COMPLEMENTAL : e.g micturation and defication reflex. sympathetic for FILLING and parasympathetic for EVACUATION N.Bboth sympathetic and parasympathetic together help acurate control over an organ's activity.
AUTONOMIC GANGLIA DEFINITION :It is the site of physiological contact between pre and post ganglionic fibers . TYPES: a) lateral (sympathetic) b) collateral (mixed) or pure sympathetic c) terminal ( parasympathetic ) Lateral( paravertebral) 23 ganglia: 3 = cervical sympathetic chain 12 = thoracic 4 = lumber 4 = sacral
Collateral:Around large .B.V as: - Caeliac ganglion - Superior mesentric ganglion - Inferior mesentric ganglion Terminal(in the wall of organ, no post-ganglionic as vagus or may be present very short post-ganglionic fiber
Pathway of pre-ganglionic sympathetic fibers: 1- May synapse in first sympathetic chain ganglion, it enters. 2- Synapsing in other sympathetic chain ganglia up or down. 3- Synapse in collateral ganglia. 4- Synapse in substance of adrenal medulla itself.
Function :1) Distributing center: Sympathetic Parasympathetic 1 : 32 1:9 or 1:2 ?? 2) Relay station between pre and post ganglionic fiber Localization :To diagnose site of relay, by Nicotine test: (Langlay's test) painting the ganglia with large doses of nicotine to block the site of relay, after that if it gives no post - ganglionic response = relay Cervical Division of sympathetic
DESTRIBUTION OF SYMPATHETIC NERVOUS SYSTEM 1) CERVICAL DIVISION: Origin: It arises from lateral horn cell of Ti and T2 and end in superior cervical ganglion I) EYE : a) dilatorpupilllary muscels = pupillary dilatation = Mydriasis b) Tarsal m.=elevation of eye lid = widening of eye superior inferior c) Muller's m. = Exophthalamos = Protrusion of eye ball in animals d) Blood vessels of eye = V.C e) relaxation of the ciliary muscle for vision
II) SALIVARY GLANDS : a) Secretion of small amount of saliva, rich in organic matters (enzymes) i.e viscus saliva . b) Squeezing around acinin of salivary glands push saliva outside III) SKIN : a) Erector pilae m = erection of hairs b) Vaso-conistriction of blood vessels = pallor c) Sweat :Secretion = mental sweat. IV) Cerebral blood vessels = vaso-conistriction
HORNER'S SYNDROME It IsCerviaclSympathectomy: characterized by : 1-PTOSIS : drop of upper eyelid. 2- MIOSIS :pupillaryconstriction . 3- ANHYDROSIS :dryness of skin 4-Emrophthalamos 5- Flushing of the face ALL THESE EFFECTS ARE AT SAME SIDE OF LESHON
2) CARDIQ-PULMONARY DIVISION : Segments and end in 3rd cervical and upper 4 thoracic ganglia I)HEART : increase all cardiac prosperities as: - positive inotropic effects = ↑ contractility - positive chronotropic effect = ↑ Heart rate. - = ↑ Conductivity - = ↑ Excitability II) CORONARY BLOOD VESSELS vasodilatation III) LUNG : a) bronco-dilatation . b) inhibits bronchial glands secretion of mucous IV) PULMONARY BLOOD VESSELS: vasoconstriction.
A) Greater Splanchic Nerve : it supplies the abdomen e.g : (From T5–T9, relay in caeliac ganglion) a) wall of G.I.T → relaxation of its walls = retention ↓ motility. b) sphincters → its contraction e.g pyloric sphincter of stomach c) liver → glycogenolysis = glycogen converted to glucose . d) adrenal medulla → release of epinephrin and nor epinephrine . e) spleen → contraction & release of RBCs in case of heamorrhage f) adipose tissues → lipolysis . g) inhibite the intestinal juice secretion h) relaxation of gall bladder and contraction of its sphincter. N.B Stimulation of greater splanchic nerve causes two peaks rise in blood pressure : a) First rise due to V.C of visceral blood vessel b) Second peak due to release of catecholamin into blood.
ADRENAL MEDULLA: Supplied by pre-ganglionic sympathetic fibers (greater splanchnic nerve). The circulating catecholamin have same effects of direct sympathetic stimulation, but more prolonged , So body organs can be stimulated by 2 ways, Nervous (direct) & Hormonal (indirect), Also catecholamines can stimulate sites not supplied by direct sympathetic nerves .
N.B adrenal meddulla is modified by sympethetic ganglion because : 1- No post-ganglionic fibers 2- Causes release of 80% epinephrin. 20% nor epinephrin. N.BSelective secretion of adrenal medulla: a) More epinephrine in unexpected stresses as haemorrhaege b) More nor-epinephrine in familiar stresses as hypoxia
B) Lesser splanchnic nerve: From LI - L3, relays in inferior mesentric ganglion It supplies the pelvis e.g :- a) Rectum → retention of stool (+) of internal anal sphincter b) Urinary bladder → retention of urine by relaxation of its wall and contraction of internal uretheral sphincter. c) Sex organs → ejaculation . External genitalia: In males : Inhibition of erection (v.c of erectile tissue)-Ejaculation of semen (contraction of vas deferens, prostate and ejaculatory duct( In females: Contraction or relaxation of female genital organ according to the stage of menstrual cycle and level of hormones in blood. N.B Small splanchnic nerve (from T10 – T12, relayes in caeliac and superior mesentric ganglion(
4- SOMATIC DIVISION : (Orbelli phenomenon( It is sympethetic supply of limbs, upper limbs (T4- Ts) lower limbs (T10T12), both relay in sympathetic chain = Sympethetic stimulation delays fatigue of muscle due to vasodilatation of skeletal blood vessels
ORGANS SUPPLIED BY SYMPATHETIC ONLY : 1- Ventricles (vagal escape). 2- Skin structures 3- Skeletal B.V. 4- Dilator pupillary muscles . 5- Adrenal medulla
ORGANS SUPPLIED BY PARASYMPATHETIC 1- Constrictor pupillary muscle . 2- Oesophagus . 3- Gastric glands . 4- Erectile tissue . N.B Sympethetic → causes V.C of all blood vessels, except 1. Coronaries. 2. Skeletal blood vessels.
DISTRIBUTION OF PARASYMPATHETIC I- CRANIAL DIVISION : A) Oculomotor nerve ( III N ): It arises from occulomotor nucleus , relays in ciliary ganglion FUNCTION : responsible for near visions
During fixation of eyes to near object, III nerve causes : 1) Contraction of ciliary muscle → Increases convexity of the eye lens . 2) Contraction of medical rectus muscle → medial convergence of both eyes together. 3) Contraction of constrictor pupillae muscle → papillary constriction
B) Fascial Nerve (VII N): It arises from superior salivary nucleus, relays in sphenopalatine ganglion. FUNCTION : secretion of tears and saliva which is watery, poor in enzymes and big in amount . C) Glossopharyngeal Nerve (IX N): It arises from inferior salivary nucleus 9 relays in optic ganglion . FUNCTION : secretion of saliva
D) Vagus Nerve (XN): 75% of parasympathetic fibers of the body are the vagus nerve. It arises from dorsal nucleus, relays in terminal ganglia. FUNCTION : 1- Inhibition (supression) of heart rate and contractility. 2- Broncho-constriction and inhibition of inspirartory center and secretion of mucous from bronchial glands. 3- Stimulation (excitation) of G.I.T motility and secretions .
EFFECT OF VAGUS NERVE 1-) ON HEART * Inhibits all cardiac roperties, but it does not supply the ventricles (vagus escape). * Tonic (continuous) effect on the heart , which is more marked in athelets. * Coronary vaso-constriction (V.C ) . 2) ON LUNGS: Mentioned before . 3) ON G.I.T: * Evacuation of food (stimulation of G.I.T . motility ). * Evacuation of gall bladder. * Stimulates secretion of: gastric juice , bile , pancreatic juice and mucus (Brunner's glands) * Increased hepatic blood flow. N.B Vagus nerve has no post-ganglionic fibers
WHY IT'S CALLED VAGUS ? Because it has :- 1- Afferent & efferent 2- Stimulatory & inhibitory 3- Widely distributed
II- SACRAL DIVISION OF PARAS YMPATHETIC ( nerve erigentis) It is 82 ,3,4 and called pelvic nerve and relays in hypogastric ganglia. FUNCTION : 1- It supplies urinary bladder → causes micturation 2- distal 2/3 of large intestine and rectum → causes defecation 3- Male and female sex organs → erection by vasodilatation of blood vessels of penis (♂) or clitoris (♀)
MICTURATION: Pelvic nerve causes contraction of wall of urinary bladder and relaxation of internal uretheral sphincter → passage of urine
DEFECATION : pelvic nerve causes contraction of wall of rectum and relaxation of internal anal sphincter → passage of stool N.B External uretheral or anal sphincters are not under autonomic control but under somatic control via pudendal nerve . N.B Internal sphincter is more important than external sphincter because it is smooth muscle i.e fatigue resistant, while external sphincter is skeletal muscle i.e fatigable .
CHEMICAL TRANSMITTERS DEFINITION : it is the substance which transmits the nerve impulse from pre - synaptic to post - synaptic membrane . MECHANISM : Arrival of nerve impulse to Pre-synaptic membrane → causes Ca+ uptake by acetyl choline vesicles → causes swelling and rupture of vesicles → causes release of acetyle choline which can cross the synaptic cleft → formation of acetylcholin - receptor complex → Increase Na permeability → Depolarisation Action potential This Causes Propagation of Nerve Impulse
TYPES OF NERVE ENDINGSADRENERGICCHOLINERGIC(nor adrenaline)(ac . Choline( I ) Cholinergic neurotransmission :- ( six steps ) 1- Synthesis of acetyl choline :-( In cytoplasm) choline + acetyl CoA CAT Ach + CoA. ( choline - acetyl - transferase) 2- Storage of acetyl choline in vesicles In the synaptic vesicles . 3- Release of Acetyl choline :- Ca++ channels in the presynaptic membrane opens → Ac.ch. Release by exocytosis 4- Binding to receptors . 5- Degradation of Ac.ch. choline Ac.ch. choline + acetate esterase 6- Recycling of choline Into the neurone for resynthesis of Ac .ch.
SITES OF RELEASE OF ACETYL CHOLINE 1- Autonomic ganglia (i.e all preganglionic fibers) 2- All parasympathetic post - ganglionic fibers . 3- Some sympathetic post - gangljpnic as sweet glands and blood vessels of skeletal muscles. 4- M.E.P = motor end plate (i.e neuro - muscular junction) 5- Adrenal medulla (pre ganglionic ) 6- C.N.S .
A) Muscarinic receptors Sites : In cardiac muscles, smooth muscle and exocrine glands . Subtypes : Ml , M2 , M3 and M4 . -Some sympathetic post-ganglionic as sweet glands and blood vessels of skeletal muscles. - M.E.P = motor end plate (i.e neuro - muscular junction) - Adrenal medulla (pre ganglionic ) - C.N.S . Ml : in autonomic ganglia, CNS and gastric mucosa M2 : in cardiac cells and smooth muscles . M3 : in smooth muscles and secretory glands . M4 and M5 : unknown sites .
Functions of muscarinic receptors It has prolonged reseponse, lasts for seconds, either exitation or inhibition : 1- Cardiac inhibition ( slow heart rate.) 2- Broncho-constriction . 3- Salivary secretion 4- Increases G.I.T secretion and motility. 5- Pupillary constriction . 6- Contraction of ciliary muscle. 7- Contraction of urinary bladder and rectum .
B) Function of Nicotinic Receptors It has short timed receponse only exitatory : 1- Help ganglion transmission . 2- Secretion of epinephrine and nor-epinephrine from Ad. Medulla. 3- Stimulates N.M.J (MEP) to produce skeletal muscle contraction
FATE (REMOVAL) OF AC CHOLINE .By choline-estrase enzyme 2 types. True pseudo (false) - present in nerve –endings - present in plasma. specific only for Ac - non specific, can act on any ester - highly potent (strong) - less potent.
PARASYMPATHOMIM ETIC DRUGS Acts By Two Ways : A) Direct : on tissues as muscarine, nicotine in small dose and carbachol. B) Indirect : anticholinesterases as DFP and Eserine (war gas)
Anti cholinesterases : Two types : a) Reversible : short acting e.g Eserine : generalized i.e. ↑ both muscarinic and nicotinic actions. Prostigmine: Nicotinic i.e ↑ skeletal muscles MEP activity = used in treatment of myasthenia gravis . b) Irreversible : long acting drugs i.e toxic, called nerve gases, or insecticides as DFP which causes paralysis of motor functions → difficulty in breathing → death
PARASYMATHOLYTIC DRUGS Mechanism of action : 1) Persistent depolarization 2) Competitive inhibition as curare. Types : A) ganglion blockers -Nicotine in large doses - Hexamethonium They cause paralysis of autonomic ganglia by persistant depolarization . B) post - ganglionic blockers -Atropine C) MEP blockers - Curare - Botulinum - Flexidil - Succinyl cholin . ( persistent depolarization)
Curare :- acts by competitive inhibition to Ac.ch . It can be used together with succinyl choline as muscle relaxants ATROPINE (anti-muscarinic drug ): ACTION : a) ON THE EYES :- Mydriasis and cycloplegia(loss of ability for near vision) b) ON SALIVARY GLANDS :- Dryness of mouth c) ON G.I.T :- Decrease motility = antispasmodic d) ON RESPIRATION : - Block secretions in respiratory tract e) ON C.V.S :- Tachycardia = ↑ heart rate . f) ON URINARY TRACT :- ↓ motility of urinary bladder .
Effect of injection of Ac.ch. after Atropine on A.B.P Nicotinic receptors in adrenal medulla unblocked rise in A.B.P CLINICAL USES OF ATROPINE 1- Fundus examination → Mydriasis 2- Bronchial asthma → Bronchodilatation . 3- Treatment of colic →↓ motility of G.I.T . 4- pre anaethetic drugs to prevent cardiac arrest. 5- Befor surgery → to block respiratory secretions
ADRENERGIC TRANSMISSION 5 STEPS : Hydroxylase enz. 1- Tyrosine DOPA (In cytoplasm). Dopa dopamine . 2- Storage of nor epinephrine in vesicles :- OH Dopamine Nor. epinephrine ( In synaptic vesicles .) N.B In adrenal medulla only: CH3 Nor - epinephrine epinephrine . 3- Release of nor-epinephrine :- Into the synapse. 4- Binding by receptors : either post-synaptic ( on the effector organ) or pre- synaptic receptors ( on nerve endings.) 5- Removal of nor- epinephrine ( Fate ) .
SITES OF RELEASE OF CATECHOLAMINES 1- Adrenergic endings :- only nor - adrenaline . 2- Adrenal medulla :- causes release of : 80% epinephrine 20% nor-epinephrine FATE OF CATECHOLAMINES 1- Active reuptake = 80-90% back into ad. vesicles. (Na-k Atpase sys.) 2- Destruction = 7 % by MAO (oxidation) COMT (methylation) 3- Excretion as such = 3 %
ADRENERGIC RECEPTORS (ALQUISTE) α1 : STIMULATORY a) V.C b) stimulation of sphincters . α2 :- INHIBITORY 0 a) relaxation of walls of G.I.T b) pre - synaptic inhibition of release of nor epinephrine (-ve feedback) βl :- STIMULATORY (+) a) heart +ve increase H.R & contraction b) adipose tissue = lipolysis c) renin - angiotensin . system = ↑ ABP. β2 :-INHIBITORYO (–)relaxation of smooth muscles in : 1- bronchi = bronchodilatation . 2- blood vessels = V.D in skeletal blood vessels & coronaries.
N.B β1 receptors are stimulated equally by epinephrine and nor-epinephrine B2 receptors stimulated more by epinephrine than N.E β2 adrcnoreceptors : tow groups α 1 & α2: αl receptors have high affinity for phenyl-ephrine present on post.synaptic membrane of effector organ . α2 receptors have high affinity for clonidine. present on Pre-synaptic nerve endings to control release of nor-epinephrine (causes its inhibition). N.B β2 pre-synaptic receptors stimulate NE release, both a 2 and β2 receptors are called pre - synoptic receptors.
RECEPTOR STIMULANTS α Receptors stimulated by : nor - adrenaline ]- adrenaline} isoproterenol β Receptors stimulated by : isoproterenol J. adrenalin]- nor - adrenaline N.B nor - adrenaline, has a more pressor effect because it acts mainly on α due to receptor sensitivity. RECEPTOR BLOCKERS : α Blockers : ergot alkaloids . β Blockers : inderal .(Propranolol.) N.B In G.I.T inhibition of the wall is by α2 and may be β2 receptors. While stimulation of sphincters only by al receptors (not β1 ). N.B α is stimulatory except on G.I.T, it is inhibitory While β is inhibitory except on heart, it is stimulatory.