Genital prolapse
Genital prolapse. DISPLACEMENTS OF THE UTERUS. The uterus is normally anteverted,anteflexed Version: is the angle between the longitudinal axis of cervix, and that of the vagina. Flexion: is the angle between the longitudinal axis of the uterus, and that of the cervix.


Genital prolapse
E N D
Presentation Transcript
Genital prolapse DISPLACEMENTS OF THE UTERUS
The uterus is normally anteverted,anteflexed Version: is the angle between the longitudinal axis of cervix, and that of the vagina. Flexion:is the angle between the longitudinal axis of the uterus, and that of the cervix.
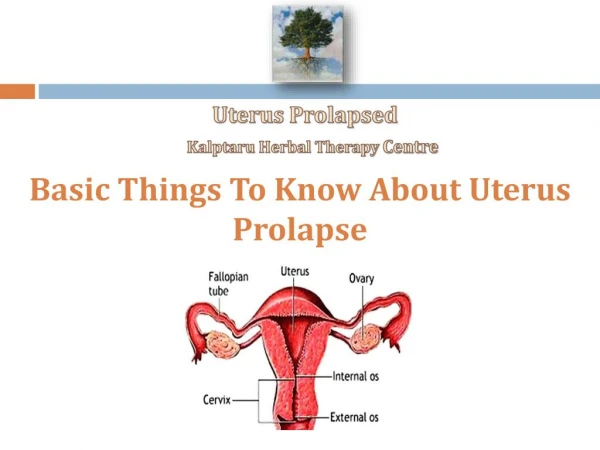
Downwards Displacement (Genital Prolapse) Genital prolapse is the descent of one or more of the genital organ (urethra, bladder, uterus, rectum or Douglas pouch or rectouterine pouch”) through the fasciomuscular pelvic floor below their normal level. Vaginal prolapse can occur without uterine prolapse but the uterus cannot desent without carrying the vagina with it.
Varieties of prolapse: Vaginal Prolapse: 1) Anterior vaginal wall prolapse: a. Prolapse of the upper part of the anterior vaginal wall with the base of the bladder is called cystocele b. Prolapse of the lower part of the anterior vaginal wall with the urethra is called urethrocele. c) Complete anterior vaginal wall prolapse is called cysto-urethrocele.
2) Posterior vaginal wall prolapse: a) It is called rectocele if the anterior wall of the rectum is also prolapsed with the middle third of the posterior vaginal wall. b) It is called entrocele (hernia of the pouch of Douglas) if the upper third of the posterior vaginal wall descends lined by the peritoneum of the Douglas pouch and containing loops of the intestine
3) Vault prolapse: (descent of the vaginal vault, where the top of the vagina descends )or inversion of the vagina) after hysterectomy. * Vault prolapse is more likely to occur after subtotal than after total hysterectomy.
II) Uterine prolapse: 1)Utero-vaginal (the uterus descends first followed by the vagina): This usually occurs in cases of virginal and nulliparous prolapse due to congenital weakness of the cervical ligaments. 2) Vagino-uterine (the vagina descends first followed by the uterus):This usually occurs in cases of prolapse resulting from obstetric trauma.
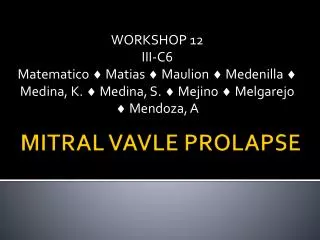
Degrees of uterine prolapse 1st degree: The cervix desent below its normal Ievel on straining but does not protrude from the vulva. N.B.: The extemal os of the cervix is at the level of the ischial spines. 2nd degree: The cervix protrudes from the vulva on straining 3rd degree: (Complete procidentia) the whole uterus is completely prolapsed outside the vulva and the vaginal wall becomes most completely inverted over it. Enterocele is usually present.
Degrees of uterine prolapse • 1st degree-2nd degree-3rd degree
Etiology of prolapse The primary cause of prolapse is weakness of the supporting structures of the uterus and vagina, usually as a result of the trauma of childbirth
Predisposing Factors: 1. Weakness of the pelvic cellular tissue: The cervical ligaments which act as the main support for the uterus may become weakened by the following: a) Obstetric trauma b) Congenital weakness c) Postmenopausal atrophy 2)Injury of the pelvic floor
Symptoms of prolapse: • Before actual prolapse. the patient feels a sensation of weakness in the perineum. particularly towards the end of the day. 2. Later the patient notices a mass which appears on straining. and disappears when she lies down. 3. Urinary symptoms are common and trouble some even with slight prolapse: a) Urgency and frequency by day. b) Stress incontinence. c) Inability to micturate unless the anterior vaginal wall is pushed upwards by the patient's fingers. d) Frequency and scalding day and night when cystitis develops .
4. Rectal symptoms are not so marked. The patient always feels heaviness in the rectum and a constant desire to defoecate. Piles develop from straining. 5. Backache, congestive dysmenorrhoea and menorrhagia are common. 6. Leucorrhoea is caused by the congestion and associated by chronic cervicitis.
Treatment of Prolapse A) Prophylactic treatment for Obstetric prolapse: 1. Proper ante-natal care (before delivery):The pelvic floor should be both strong and elastic. It is strong to help internal rotation of the fetal head in the second stage of labour (Gutter like action) and is elastic, so that the baby can pass through painlessly causing the least amount of trauma to the pelvic floor.
2. Proper intra-natal care (during delivery):Avoid aetiological factors as straining during the first stage(before full cervical dilatation); avoid the application of forceps before full cervical dilatation; episiotomy should be done when indicated to avoid hidden perineal lacerations; and avoid fundal pressure to deliver the placenta.
3. Proper post-natal care (after delivery): Accurate repair of perineal tears or episiotomies, avoidance of occurrence of R.V.F. by postural treatment (daily time rest, relaxation on face, knee chest position) correction of retroversion during the puerperium with the use of knee chest position or pessaries, encourage pelvic floor exercises and other postnatal ex's, prevent puerperal constipation in order to avoid strong bearing down efforts while the supporting ligaments of the uterus are slack, and care of general health to prevent debility and bad general health.
B) Palliative treatment: palliative treatment by wearing a pessary is indicated in the following conditions: 1)Slight degrees of prolapse in young patients. Operation should be postponed until the woman has had a sufficient number of children as long as the symptoms are mild. 2) Prolapse of the uterus in early pregnancy. The pessary is worn until the end of the fourth month until size of the uterus will be sufficient to prevent its descent. 3) Contraindications to operations as lactation, severe cough , or patients refusing surgical repair. 4) Bad surgical risks as old patient with advanced diabetes or severe hypertension.
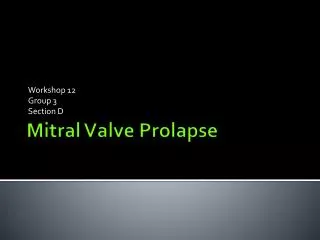
Ring pessaries: A pessary of suitable size is introduced in the vagina above the level of the levator anie muscies. It stretches the redundant vaginal wall and prevents descent of the uterus. The "cup and stem" pessary : Is used if the patient's pelvic floor are so weak or lacerated that a ring pessary cannot be retained in the vagina. Whatever type of pessary is used, this method of treatment is at its best only a temporary method to give relief of symptoms. There is always the drawback of a foreign body in the vagina, which is liable to cause leucorrhoea and if neglected may even ulcerate into the wall of the vagina. Pessaries used in prolapse
A pessary is a device which is inserted into the upper part of the vagina to provide support to the pelvic structures. The majority of pessaries are made of silicone and come in a number of shapes and sizes. A pessary needs to be inserted by a medical professional and can be kept in place for 3-4 months, after which it will require changing. When inserted properly, a woman should not be able to feel a pessary. Pessaries provide a temporary solution to prolapse symptoms for pregnant women, women who have recently given birth or for women who are awaiting surgery. Pessaries can also be used permanently by women who do not wish to have surgery or who are unsuitable candidates
Precautions during wearing a pessary: The patient is instructed to have a daily vaginal douche, and every month the pessary is removed, cleaned, the vagina examined for any signs of pressure and the pessary then reintroduced. If the pessary is made of rubber it should be changed every three months.
c)Actual treatment: Physiotherapeutic lines: indicated in: 1. Early and mild cases. 2. As a prophylactic measure after delivery. 3. Alleviation in more severe cases (pre-and post operative treatment). Aims out of P.T. treatment • To establish the awareness of the function pubococcygeus and pelvic supports & To strength the pubococcygeus muscle.
Physical therapy treatment: Is divided into two phases: Muscle re-education: Is important as the patient lack awareness of the function of the pubococcygeus muscle, it includes: • Muscle re-education for pubococcygeus muscle • Biofeedback [Kegel perineometer and EMG biofeedback .Mid-stream urine flow (stop test) .Cyriax method Resistive exercises for pubococcygeus muscle: • An inflated cuffed catheter • Vaginal cones
a)Muscle re-education of pubococcygeus muscle:Pelvic floor exercises b)Biofeedback (Kegel perineometer and EMG biofeedback): Kegel perineometer provides the patient by powerful sensory and visible biofeedback, is able to measure pubococcygeus muscle up to 100 mmhg so that changes in pelvic floor strength can be measured.,
EMG biofeedback Provides the patient by sensory, visible and auditory biofeedback EMG biofeedback is useful in both increase the level of pubococcygeu muscle activity and improving the ability of the muscle to relax on volition ,EMG devices and perineometers appears to be useful tools for evaluation,& treatment) of pelvic floor dysfunction.
* Cyriax method Cyriax method of treatment for stress incontinence is also suitable for early cases of genital prolapse. This method aims to strength: pubococcygeus, gluteal, anal, and abdominal muscles. . The patient is asked to lie in crock-lying position, to breathe in deeply from her nose, and at the same time contract pubococcygeus, gluteal, anal and abdominal muscles, this is associated with drawing all internal viscera up towards the diaphragm, then she will asked to relax and expire air from her mouth with a sigh .