Download
1 / 18
180 likes | 277 Vues
Explore the impact of health disparities on minority groups in the US, factors contributing to inequalities, and the initiatives like healthcare reform and global health policies aimed at reducing disparities. Learn about the societal and personal costs of disparities and the importance of addressing them for better healthcare outcomes. Discover how government funding and advocacy efforts are working towards improving global health. Stay informed on the latest developments and strategies for promoting health equity.

E N D
Health Disparities • The U.S. Department of Health and Human Services defines “health disparities” as differences in the occurrence, frequency, death, and burden of diseases and other unfavorable health conditions that exist among specific population groups, including racial and ethnic minority groups. • www.minorityhealth.hhs.gov
In March 2003, the Institute of Medicine issued a report finding overwhelming evidence that racial and ethnic minorities suffer disparities in health care and concluding that the real challenge lies not in debating whether disparities exist, but in developing and implementing strategies to reduce and eliminate such disparities.
Research shows that minorities are: • in poorer health • experience more substantial obstacles to receiving care • are more likely to be uninsured • are at greater risk of receiving care of poor quality than other Americans
National Healthcare Disparities Report, 2003 • Minorities are more likely to be diagnosed with late-stage breast cancer and colorectal cancer compared with whites. • Patients of lower socioeconomic position are less likely to receive recommended diabetic services and more likely to be hospitalized for diabetes and its complications. • When hospitalized for acute myocardial infarction, Hispanics are less likely to receive optimal care. • Many racial and ethnic minorities and persons of lower socioeconomic position are more likely to die from HIV. Minorities also account for a disproportionate share of new AIDS cases. • The use of physical restraints in nursing homes is higher among Hispanics and Asian/Pacific Islanders compared with non-Hispanic whites. • Blacks and poorer patients have higher rates of avoidable hospital admissions (i.e., hospitalizations for health conditions that, in the presence of comprehensive primary care, rarely require hospitalization).
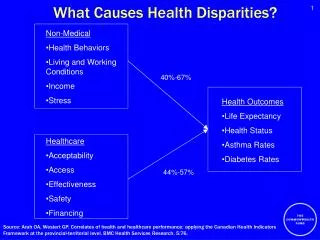
Factors contributing to differences in health care include • poverty • lack of access to health care • lack of health insurance • language and literacy barriers • poor expectations of the result of treatment, the doctors, and/or the health-care system
Disparities come at a personal and societal price • Health care disparities are costly. • Poorly managed care or missed diagnoses result in expensive and avoidable complications. • http://www.americashealthrankings.org/2009%5Creport%5CAHR2009%20Final%20Report.pdf
US Healthcare Reform Patient Protection and Affordable Care Act (PPACA)- signed into law March 23, 2010 • The law includes a large number of health-related provisions to take effect over the next four years, including expanding Medicaid eligibility, subsidizing insurance premiums, providing incentives for businesses to provide health care benefits, prohibiting denial of coverage/claims based on pre-existing conditions, establishing health insurance exchanges, and support for medical research
US Global Health Policy and Advocacy Raising awareness and funds for global health
US government funding for Global Health • President Bush created and increased funding for PEPFAR and President’s Malaria Initiative but cut funding for Child Survival, the Global Fund to Fight AIDS, Tuberculosis and Malaria, and core development funding for education and clean water initiatives. President Obama is changing this, but slowly. • http://www.kff.org/globalhealth/7881.cfm
Successes • President Obama overturned the “Global Gag Rule” that was reinstated by former President GW Bush during his presidency • Increased funding for Global Health through the development of a Global Health Initiative, coordinating government offices and placing specific attention on maternal and child health outcomes globally • US Healthcare reform
Global Health Initiative • Through the Global Health Initiative (GHI) the United States will invest $63 billion over six years to help partner countries improve health outcomes through strengthened health systems • with a particular focus on improving the health of women, newborns and children through programs including infectious disease, nutrition, maternal and child health, and safe water. • www.globalhealth.gov
FY2011 State/Foreign Operations Appropriations Bill • On July 29, 2010 the Senate Appropriations Committee marked up the FY 2011 State/Foreign Operations Appropriations bill. • The Senate marked level of the Department of State, Foreign Operations and Related Programs Appropriations Bill is $54.06 billion; $2.6 billion below the President’s request and $5.29 billion above the FY 10 enacted levels.
The FY 11 President's request for total global health funding was $8.513 billion. After House Subcommittee mark-up, total global health funding stands at $8.25 billion; a $263 million decrease from the President's request. • Senate mark-up of the bill left global health funding at $8.239 billion. • This includes: Maternal and Child Health: $641 million including $33.1 million for programs to eradicate Polio and an additional $100 million allocated for nutrition (House Mark: $750 million including up to $100 million for nutrition; FY10: $549 m including $75 m for nutrition). • Family Planning: $700 million for all family planning and reproductive health accounts, including and $55 million in contributions to the United Nations Population Fund (House mark: $735 million total. $675 m for USAID family planning and $60 m in contributions to the United Nations Population Fund; FY10: $648.5 m including contributions to UNFPA).
Malaria: $635.5 million (House mark: $615 million; FY 10: $585m). • Tuberculosis: $230 million (House mark $240 million; FY 10: $225 m). • Neglected Tropical Diseases: $100 million; President’s request $155 million (House mark $80 m; FY 10: $65m). • HIV/AIDS funding under the State GHCS account is broken down as follows: • HIV/AIDS Bilateral: $5.85 billion, which is equal to the President’s request (House mark: $5.050 billion; FY 10: $4.959 billion). • Global Fund (foreign operations only): $800 million, which is $100 million above the President’s request (House mark: $825 million; FY10: $750 million).
FY2012 • On July 27, 2011: According to an analysis by the Global Health Technology Coalition (GHTC), the bilateral assistance account is cut by $3.5 billion from FY2010 levels, and is $4.8 billion below the FY2012 President’s request. For GHI, the House panel earmarked $7.1 billion for FY2012, which is $1.6 billion less than Obama's request.
Millennium Development Goals • Eliminate gender disparity in primary and secondary education at all levels by 2015 • Reduce by two thirds the mortality rate among children under five • Reduce by three quarters the maternal mortality ratio www.commitinseptember.com
ONE Vote ’08- Success • $30 million ONE bipartisan campaign to make global health and extreme poverty foreign policy priorities in the 2008 election www.onevote08.org/aboutone.php