Download
1 / 27
290 likes | 719 Vues
HAEMODYNAMIC MONITORING Michael L. Cheatham, MD, FACS, FCCM Director, Surgical Intensive Care Units Orlando Regional Medical Center Orlando, Florida, USA. OBJECTIVES. To discuss the various monitoring technologies that may be used in the patient with IAH / ACS

E N D
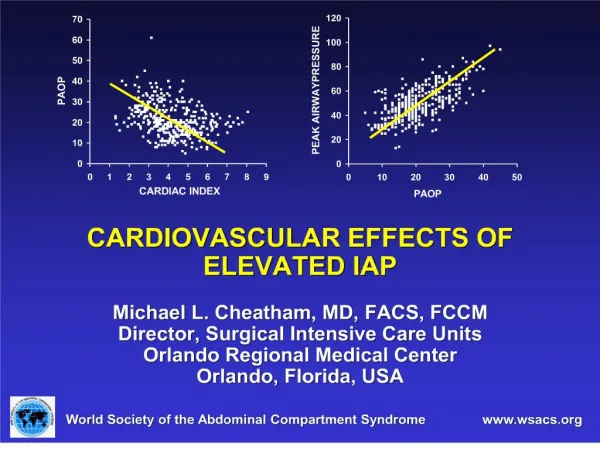
HAEMODYNAMIC MONITORING Michael L. Cheatham, MD, FACS, FCCM Director, Surgical Intensive Care Units Orlando Regional Medical Center Orlando, Florida, USA
OBJECTIVES • To discuss the various monitoring technologies that may be used in the patient with IAH / ACS • To describe the relative merits and limitations of the various monitoring techniques • To present an evidence-based medicine approach to haemodynamic monitoring and resuscitation in the patient with IAH / ACS
INVASIVENESS TECHNOLOGY COMPARISON
Technology Preload Contractility Afterload Oxygen Transport Cost Continuous TD PAOP, CVP, RVEDVI CO, RVEF SVR SvO2 $$$ Bolus TD PAOP, CVP CO SVR $ Pulse Contour GEDVI, SVV CO SVR $$ Lithium Dilution SVV CO SVR $$$ INVASIVENESS Esophageal Doppler FTc CO $ Bioimpedance CO $$$ Clinical Examination TECHNOLOGY COMPARISON Only the technologies shown have been evaluated in IAH / ACS
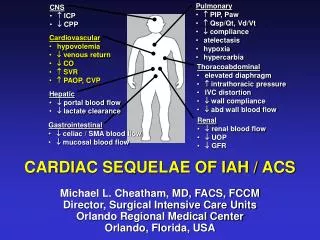
CLINICAL EXAMINATION • IAH / ACS can be difficult to detect • Clinical exam cannot be relied upon to diagnose elevated IAP • Sensitivity of experienced clinicians is less than 50% • IAP monitoring is essential to identifying IAH / ACS and reducing its associated morbidity and mortality
PULMONARY ARTERY CATHETER (PAC) • Originally described by Swan & Ganz (1972) • The “gold standard” for the next two decades • Allows assessment of • Preload • Pulmonary artery occlusion pressure (PAOP) • Central venous pressure (CVP) • Contractility • Cardiac output (CO) • Afterload • Systemic vascular resistance (SVR)
BOLUS THERMODILUTION • CO is determined by measuring a “thermodilution curve” following injection of iced saline • Accuracy is dependent upon multiple factors • Respiratory cycle • Injection technique • Regular heart rate • Proper catheter positioning, transducer calibration, and waveform interpretation are essential
THE LIMITATIONS OF THE PAC • Requires an invasive right heart catheter • Risks of pneumothorax, hemothorax, arrhythmia, infection • Use is based upon several assumptions: • Intermittent measurements reflect a patient’s continuously changing hemodynamic state • PAOP & CVP accurately reflect end-diastolic volume • Ventricular compliance is unchanging
THE PAOP ASSUMPTION Is ventricular geometry unchanged? Is ventricular compliance unchanged? Catheter properly positioned? Is there mitral valve disease? Preload = LVEDV = LVEDP = LAP = PAOP PAOP is accurate ONLY when these potential sources of error have been eliminated Are intrathoracic or intra-abdominal pressures elevated?
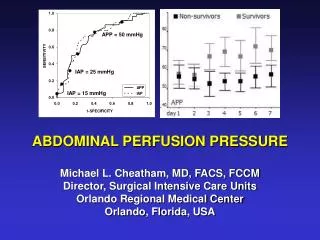
TRANSMURAL FILLING PRESSURES • Resuscitation to arbitrary, absolute PAOP or CVP values should be avoided • Transmural pressures may be of greater accuracy PAOPtm = PAOPee - Ppl CVPtm = CVPee – Ppl • Substituting IAP for Ppl may provide a rapid bedside estimate of transmural filling pressure
IS THE PAC FLAWED OR ARE WE? • Various studies have demonstrated that… • 47% of physicians cannot derive basic hemodynamic information from a PAC • 33% cannot identify a PAOP tracing • 33% cannot describe how to increase a patient’s oxygen delivery • Is it any surprise that prospective trials have failed to demonstrate a survival benefit with the use of this device?
THE EVOLUTION OF THE PAC • Mixed venous oximetry (SvO2) (1980’s) • Assessment of oxygen transport balance • Volumetric technology (1990’s) • Assessment of right heart function • Right ventricular ejection fraction (RVEF) • Right ventricular end-diastolic volume (RVEDVI) • A volumetric, as opposed to pressure-based, estimate of intravascular volume status • Superior to PAOP & CVP in predicting preload recruitable increases in CO J Trauma 1999; 46:1-7
RVEDVI IN INTRA-ABDOMINAL HYPERTENSION r = - 0.33 r = - 0.33 r = 0.44 r = 0.69
RVEDVI IN INTRA-ABDOMINAL HYPERTENSION r = - 0.33 r = - 0.33 r = 0.68
ARE WE MISSING TOO MUCH? • Significant physiologic changes may go undetected by conventional intermittent monitoring techniques • A “snapshot” in time when a “moving picture” is what is needed
CONTINUOUS THERMODILUTION • Utilizes pulsed thermal energy technology • Provides an updated hemodynamic assessment every 60 seconds • Reduces measurement variability • Automates CO measurement • Averages respiratory cycle variation • Standardizes injection technique • Provides a constantly updated assessment of patient response to resuscitation leading to more efficient, goal-directed resuscitation
CONTINUOUS THERMODILUTION • Most invasive and labor-intensive of the monitoring technologies demanding a thorough understanding of PAC monitoring principles • Provides a continuous assessment of • Preload (RVEDVI) • Contractility (CO, RVEF) • Afterload (SVR, RVEF) • Oxygen transport balance (SvO2) • Improves patient resuscitation and outcome • Appropriate for the most critically ill patients
ARTERIAL PULSE CONTOUR ANALYSIS • Estimation of SV from the arterial pressure waveform was first described almost 100 years ago • CO is proportional to the area under the arterial pressure waveform • Proposed as a less invasive alternative to the PAC • Requires only an arterial pressure catheter and a central venous catheter (CVC)
ARTERIAL PULSE CONTOUR ANALYSIS • Accuracy is dependent upon arterial resistance, compliance, and impedance • Initial calibration via iced saline thermodilution • Recalibration every 8 hours • Provides continuous assessment of • Left ventricular SV and CO • Global ejection fraction (GEF) • Global end-diastolic volume (GEDV) • Intrathoracic blood volume (ITBV) • Extravascular lung water (EVLW) • Stroke volume variation (SVV)
ARTERIAL PULSE CONTOUR ANALYSIS • A less invasive alternative to a PAC • Provides continuous assessment of • Preload (GEDVI, ITBVI, EVLW, SVV) • Contractility (CO) • Afterload (SVR) • Multiple studies have demonstrated that CO correlates better with GEDVI and ITBVI than with PAOP in the presence of elevated ITP and IAP • A viable option for minimally invasive continuous haemodynamic monitoring
OPTIMAL RVEDVI / GEDVI • Initial studies suggested an RVEDVI of 130-140 mL/m2 or GEDVI of 640-800 mL/m2 were optimal • This oversimplifies what is actually a complex and dynamic relationship • Ventricular function and compliance are constantly changing in the critically ill • RVEF / GEF must be considered when determining the optimal volume for resuscitation End-diastolic volume1 / Ejection Fraction
RVEF 0.20 RVEF 0.30 RVEDVI RVEF 0.40 CARDIAC INDEX FAMILIES OF STARLING CURVES As contractility changes, patients move to a new Starling curve and the target RVEDVI / GEDVI must change
RESUSCITATION ALGORITHM • Initially resuscitate to a RVEF-corrected RVEDVI of 100 mL/m2 • Patients with a lower RVEF are resuscitated to proportionally higher RVEDVI values • If malperfusion persists, increase the target RVEDVI by 20% • Consider vasoactive medications based upon the patient’s RVEF and SVR
RESUSCITATION ALGORITHM • Each patient should be resuscitated to the RVEDVI or GEDVI that restores end-organ function and normalizes markers of perfusion adequacy • Unnecessary over-resuscitation should be avoided • May lead to secondary ACS, lung dysfunction • PAOP and CVP may be used to guide resuscitation with the explicit understanding that transmural estimates of PAOP and CVP must be utilized
CONCLUSIONS • Haemodynamic monitoring and goal-directed resuscitation is essential to improving patient outcome from IAH / ACS • PAOP and CVP are commonly erroneous in IAH • Reliance on such parameters may lead to under-resuscitation and inappropriate therapeutic interventions • Volumetric preload estimates such as RVEDVI and GEDVI are superior to PAOP and CVP as predictors of preload-recruitable increases in cardiac output