Therapy ulcer
Therapy ulcer. of peptic. Peptic ulcer. defects of mucosa of the stomach / duodenum = mucosal damage through the lamina muscularis mucosae Clinical presentation : stomach – pain in the epigastrium shortly after meal (the patient often looses weight), nausea, anorexia


Therapy ulcer
E N D
Presentation Transcript
Therapy ulcer of peptic
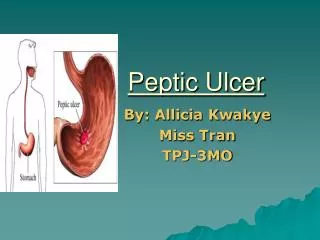
Peptic ulcer • defects of mucosa of the stomach / duodenum = mucosal damage through the lamina muscularis mucosae Clinical presentation: stomach – pain in the epigastrium shortly after meal (the patient often looses weight), nausea, anorexia duodenum – pain later after meal (fasting), often during the night, gets better after eating, the patient can gain weight
Etiopatogenesis imbalance: aggressive factors ↔ protective factors mostly- HCl, pepsin production ↑ - histamine, acetylcholine, gastrin, etc. mostly- mucus, bicarbonate, fast regeneration of the mucosa, adequate perfusion of the gastric wall protective factors ↑ - mostly the production of prostaglandins by cyklooxygenase
Etiopatogenesis - causes • Helicobacter pylori (Hp) • drugs- most frequently NSAIDs, then corticoids etc. • smoking • dietary mistakes (questionable) • psychosocial stress • genetical factors • conditions with shock, burns, head traumas • Zollinger- Ellison sy. • ..........
Diagnosis and Nonpharmacologic treatment • ezophagogastroduodenoscopia histologic check of nature of the ulcer lesions presence of Hp= microscopyhisto-morfology rapid urease testbreath test testing of Ab (in plasma and in stool) • nonpharmacol. therapy: lifestyle (sleep, ↓ stress)diet (often in smaller amounts, ↓ spicy, ↓ caffeine) no smoking
Helicobacter pylori – black bacteria on the surface of the gastric mucosa
Antisecretorydrugs (↓ productionofHCl): protonpumpinhibitors(PPI)- omeprazole H2receptor antagonists- famotidine anticholinergics (Pslytics)- pirenzepine DrugsneutralisingHCl: coloidalantacids- compoundsofAl a Mg reactiveantacids- NaHCO3 a CaCO3 Mucoprotectives: prostaglandines, sucralfate, compoundsofbismuth ATBs: amoxicillin, claritromycin, metronidazole, doxycycline; in caseoffailureoftherapy- levofloxacin, rifabutin
Proton pump inhibitors • MA – irreversible blockade of H/K-ATPase(proton pump) • most effective antisecretory drugs (inhibit the last phase of HCl secretion → effect independent from the stimulus for HCl secretion) • elevated pH in the stomach decreases the conversion - pepsinogen → pepsin • “prodrugs“ - converted into active metabolite in the parietal cells of gastric mucosa • good safety profile, good tolerance • basic pharmacotherapy for peptic ulcer
Proton pump inhibitors omeprazole:nearlycompleteblockadeofHClsecretionat rest and afterstimulus, hightherapeuticeffectivity druginteractions: diazepam, phenytoin, warfarinclopidogrel??- somestudies- might ↓ effectivityofclopidogrelbecauseofinhibitionof CYP450- administerratherpantoprazole pantoprazole, lanzoprazole: lessinteractions, suitable in polymorbid and olderpatientsesomeprazole:inovatedomeprazolewithfasteronset and longerdurationofactionNewerdrugs: ilaprazol tenatoprazol:strongesteffect, longestdurationofeffect
H2 receptor antagonists • MA - selective blockade of H2 histamine receptors → inhibition of histamine mediated HCl production (indirect effect on secretion mediated by Ach and gastrin) • ↓ effectivity than proton pump inhibitors Examples – cimetidine, ranitidine, famotidine (more effective), nizatidine - good safety profile, good tolerance - drugs of 2nd choice for treatment of peptic ulcer; loosing therapeutic role in most indications (↓ effectivity)
Anticholinergics • MA – inhibition of M1 receptors → inhibition of acetylcholine mediated HCl production • ≈ same effectivity as H2 antagonists • ADRs – consequences of ↓activity of PS – for example dry mouth, problems with vision and urination, constipation • example- pirenzepine - they lost their therapeutic role – ADRs, ↓ effectivity than proton pump inhibitors
coloidal antacids: aluminum and magnesiumhydroxide MA: weak bases → bind HCl; slightly ↑ the production of prostaglandines ADRs: - Al hydroxide: constipation, ↓ resorption of phosphates → osteomalacia; - Mg hydroxide: diarrhoea, hypermagnesemia; both- risk of interactions!! • reactive antacids: NaHCO3and CaCO3 MA: reaction with HCl, during which CO2 is formed ADRs: - flatulence, ´milk-alkali´ syndrome (hypercalcemia, nephrolithiasis, renal insufficiency, ...), in the case of NaHCO3 metabolic alkalosis !!!! Antacids – only for symptomatic treatment of dyspepsia!!!
Prostaglandines • misoprostol (analog of PGE1), enprostil (analog of PGE2) - cytoprotective and mucoprotective effect - improve the microcirculation underneath the mucosa + ↑ production of mucus and bicarbonate + ↑ regenerationof defects ADRs – diarrhoea, stomach pain, abortion, - can be used in prevention of peptic ulcer formation during NSAID treatment (for that, we have other, in most cases better alternatives)
Sucralfate • salt of sulfonated sucrose • MA: in an acidic environment it forms a protective layer on the surface of the mucus membrane and on the surface of the defect • probably stimulates the formation of prostaglandines • well tolerated • !don´t administer after administration of antisecretory drugs! • seldomly used
Bismuth • ↑secretionofmucus and bicarbonate, ↓ secretionofHCl, antibacterialeffect • ADRs – metallic taste in themouth, blacktongue and stool, !neurotoxicity (confusion, hallucinations...) nowadaysusedlessfrequently (risk ofADRs), part of 2nd lineof H. pylorieradicationtherapy
Eradication of Helicobacter pylori (needed for long-term success of pharmacotherapy of peptic ulcer in Hp positive patients)
1st linetreatment: triple therapy 7 or14 daytreatment (14 days – betterresults) • protonpumpinhibitor • claritromycin • amoxicillin– if PNC allergy - metronidazole problem – decreasingeffectivityofthetreatment (fails in approximately 25-30 % of patients)
2nd linetreatment: quadrupletherapy (in caseoffailureoftripletherapy; in patientstreatedwithmacrolidesinthepast; canbeconsidered in patientswith PNC allergy) 7 or14 daytreatment (14 days – betterresults) • protonpumpinhibitor • bismuth • metronidazole • doxycycline problem – decreasingeffectivityofthetreatment – possibilityof ↓ compliance(dosingscheme) – ADRs (mostlybismuth)
New possibilities: sequentialtherapy 10 days (5 + 5), forexample: First 5 days • protonpumpinhibitor • amoxicillin Next 5 days • protonpumpinhibitor • claritromycin • tinidazole(possiblymetronidazole??)
Failure of the therapy: Future?? :
Non-steroidal anti-inflammatory drugs (NSAIDs) and peptic ulcer NSAIDs– one of the most widely used drug groups – in roughly 25 % of chronic users can cause erosions and ulcerations in the GIT, in 2-4 % perforation or bleeding Possibilities of prevention– proton pump inhibitors or misoprostol during NSAID treatment; use of NSAIDs selectively inhibiting COX-2 Strategy – small risk of ulcer – NSAID on its own – moderate risk of ulcer – NSAID + PPI / misoprostol – high risk of ulcer – a) administer other (non-NSAID) analgesics, or b) COX-2 selectiveNSAID + PPI / misoprostol