Download
1 / 34
350 likes | 553 Vues
Assessment of Perinatal Outcome with Sustained Tocolysis in Early Labor APOSTEL-II trial Dutch trial register: NTR 1336. Carolien Roos, MD, PhD student, UMC St Radboud Dutch APOSTEL-II Collaborative Trial Group

E N D
Assessment of Perinatal Outcome with Sustained Tocolysis in Early Labor APOSTEL-II trial Dutch trial register: NTR 1336 Carolien Roos, MD, PhD student, UMC St Radboud Dutch APOSTEL-II Collaborative Trial Group Marc EA Spaanderman, Liesbeth HCJ Scheepers, Kitty WM Bloemenkamp, Annemiek Bolte, Jerome J Cornette, Johannes J Duvekot, Jim van Eyck, Joke H Kok, Anneke Kwee, Ashley Merién, Brent C Opmeer, Martijn A Oudijk, Mariëlle G van Pampus, Dimitri NM Papatsonis, Martina M Porath, Sicco A Scherjon, Ewoud Schuit, KrystyneSollie, Sylvia MC Vijgen, Christine Willekes, Ben WJ Mol, Joris AM van der Post, Fred K Lotgering
Background • Preterm birth • 75% of perinatal deaths1 • High immediate and long-term costs2 • Corticosteroids 48 hours prior to birth • improveneonataloutcome • Effect of sustained tocolysis has not • been proven3 1 Ananth et al. Epidemiology of preterm birth and its clinical subtypes. J Matern Fetal Neonatal Med 2006 2 Gilbert et al. The cost of prematurity: quantification by gestational age and birth weight. Obstet Gynecol 2003 3 Gaunekar NN, et al. Maintenance therapy with calcium channel blockers for preventing preterm birth after threatened preterm labour. Cochrane Database Syst Rev 2004; CD 004071
Hypothesis Sustained tocolysis with nifedipine reduces perinatal mortality and severe perinatal morbidity
Inclusion criteria • Diagnosis of threatened preterm • labor • Gestational age: 26 to 32+2 weeks • Corticosteroids and tocolytic • treatment for 48 hours
Exclusion criteria • Pre-eclampsia or HELLP syndrome • Intrauterine infection / fetal • distress • Lethal congenital anomalies • Maternal hypertension • Placenta previa
Intervention 12 days sustained tocolysis: Nifedipine 4 dd 20 mg orally Placebo
Methods Nifedipine 4dd 20 mg orally Placebo Randomization 48 hrs tocolysis & corticosteroids t=-2 t=0 t=12
Primary outcome • Composite adverse perinatal outcome • Perinatal death • Chronic lung disease • Intraventricular hemorrhage > grade II • Periventricular leucomalacia > grade I • Necrotizing enterocolitis • Proven neonatal sepsis
Secondary outcomes • Gestational age at delivery • Birth weight • Ventilation support (days) • NICU admission (days) • Hospital admission (days)
Statistics • To detect a reduction of 11% in • adverse perinatal outcome, • we needed to enroll 406 patients • Intention-to-treat analysis • RR and HR; 95% CI • Kaplan-Meier curve
Data are presented as mean ± SD or median (IQR: 25th to 75th percentile) # kg/m2
Data are presented as mean ± SD or median (IQR: 25th to 75th percentile) # kg/m2
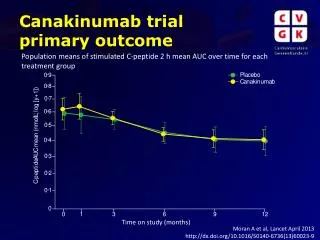
Prolongation of pregnancy (weeks) HR 1.1 (0.86 to 1.3)
Data are presented as mean ± SD or median (IQR: 25th to 75th percentile)
Data are presented as mean ± SD or median (IQR: 25th to 75th percentile)
Adverse neonatal outcome Relative Risk 95% CI Nifedipine Placebo CLD 5/201 6/205 0.85 [0.26-2.7] IVH 2/201 5/205 0.41 [0.08-2.1] PVL 0/201 0/205 NA NEC 5/201 3/205 1.7 [0.41-7.0] Sepsis 16/201 18/205 0.91 [0.48-1.7] Death 5/201 4/205 1.3 [0.35-4.7] Total 24/201 28/205 0.92 [0.53-1.5] 10 0.1 0.2 0.5 1 2 5 (favorsnifedipine) (favors placebo)
Data are presented as median and IQR (25th to 75th percentile)
Conclusion • Sustained tocolysis with nifedipine • neither prolongs pregnancy nor • improves perinatal outcome • Nifedipine is not useful beyond • 48 hours of initial tocolysis for • corticosteroid induced lung • maturation
Strengths • Large nationwide study • No additional tocolysis
Limitations • Low incidence of adverse • perinatal outcome
ACKNOWLEDGEMENT All patients who participated in the trial Trial group APOSTEL-II Kitty Bloemenkamp Annemiek Bolte Jerome Cornette Jan Derks Hans Duvekot Jim van Eyck Fred Lotgering Joke Kok Anneke Kwee Ashley Merién Ben Willem Mol Brent Opmeer Mariëlle van Pampus Dimitr Papatsonis Martina Porath Joris van der Post Liesbeth Scheepers Sicco Scherjon Krystyne Sollie Marc Spaanderman Sylvia Vijgen Christine Willekes ZonMw ACE Pharmaceuticals Pharmacy Haga Ziekenhuizen All research nurses and midwives Jannet Bakker Birgit van der Goes Viki Verfaille Sabine Logtenberg Ageeth Rosman Lida Ulkeman José Keurentjes Ineke Hamming Ina van der Wal Diana Lutjes Edwin Lubbers Clara Kolster Marjolein Verhart Marianne van der Hel Katinka Burgers Cecile Wolfs Monique Braken Vivian Ramaekers Jolande Willems Gerard Zijderveld Hanneke van de Rijt Wilma Meijer Joke van Rhee Titia Winter Wilma Keller Joyce Cantineau Nanny Konings Nelly leNoble Maartje de Reus David Borman Corine Verhoeven Corinne van der Griendt Lidewijde Jongmans Kristel Slobben Ingrid Volker Consortium Maya Kruijt Zelda van Dijk Consortium board Data Safety Monitoring Committee Ewoud Schuit PhD students All gynecologists, residents, midwives and nurses of the participating centers Leiden University Medical Center Academic Medical Center Amsterdam University Medical Center Groningen Maastricht University Medical Center Máxima Medical Center Veldhoven University Medical Center Utrecht VU University Medical Center Amsterdam Amphia Hospital Breda University Medical Center St Radboud Nijmegen Isala Clinics Zwolle Erasmus Medical Center Rotterdam
ACKNOWLEDGEMENT Patients APOSTEL-II trial Trial group APOSTEL-II ZonMw ACE Pharmaceuticals Pharmacy Haga Ziekenhuizen All research nurses and midwives Consortium board and staff All gynecologists, residents, midwives and nurses of the participating centers www.studies-obsgyn.nl/apostel2
Statistics • To detect a reduction of 11% in adverse • perinatal outcome, we needed to enroll 406 • patients • Intention-to-treat analysis • Data Safety Monitoring Committee • Interim analysis after 200 patients
Data are presented as mean ± SD, no. (%) ormedian (IQR: 25th to 75th percentile)
Data are presented as mean ± SD, no. (%) ormedian (IQR: 25th to 75th percentile)
# > grade II * > grade I