8h 16h 24h 8h
180 likes | 375 Vues
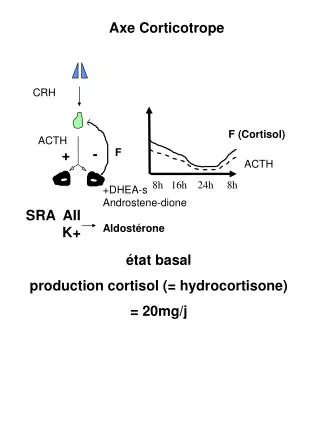
Axe Corticotrope. CRH. F (Cortisol). ACTH. -. F. +. ACTH. 8h 16h 24h 8h. +DHEA-s Androstene-dione Aldostérone. SRA AII K+. état basal production cortisol (= hydrocortisone) = 20mg/j. Axe Corticotrope. “Stress”. F (Cortisol). CRH. ACTH. ACTH. -. +. F.

8h 16h 24h 8h
E N D
Presentation Transcript
Axe Corticotrope CRH F (Cortisol) ACTH - F + ACTH 8h 16h 24h 8h +DHEA-s Androstene-dione Aldostérone SRA AII K+ état basal production cortisol (= hydrocortisone) = 20mg/j
Axe Corticotrope “Stress” F (Cortisol) CRH ACTH ACTH - + F 8h 16h 24h 8h +DHEA-s Androstene-dione Aldostérone SRA AII K+ Stress production de cortisol x2 à 10 40 à 200 mg/j
Pathologie Insuffisance surrénale périphérique Hypothalamus CRH Séméiologie: Hypophyse - ACTH mélanodermie Corticosurrénale Insuffisance minéralocorticoide glucocorticoide (androgènes) Aldostérone Cortisol DHEA-s
Pathologie Insuffisance surrénale centrale Hypothalamus CRH Séméiologie: Hypophyse - ACTH mélanodermie Corticosurrénale Insuffisance minéralocorticoide glucocorticoide (androgènes) Cortisol DHEA-s
Axe Corticotrope explorations CRH F (Cortisol) ACTH - F + ACTH 8h 16h 24h 8h F plasmatique? à 8h: si on cherche une insuffisance mais peu discriminant (que si très bas<200 nmol/l) élimine insuffisance si >580 nmol/l à 24h: si on cherche une hypersecrétion (mais difficile à prélever sauf hospitalisation)
Axe Corticotrope explorations II CRH F (Cortisol) ACTH - F + ACTH 8h 16h 24h 8h FLU/24h reflète la moyenne du cortisol libre/24h très bon paramètre pour recherche hypersecrétion bon aussi pour insuffisance problème de la qualité du recueil urinaire (créatininurie/24h)
Axe Corticotrope explorations III dynamiques: stimulation test au Synacthène CRH ACTH ACTH - F + + F (Cortisol) 580 nmol/l T0 T60
Axe Corticotrope explorations III dynamiques freinage par dexamethasone Dex CRH - ACTH - F + F (Cortisol) 100 nmol/l 23h 8h Dex
CORTICOTHERAPIE CRH Corticoïdes ACTH F (Cortisol) ACTH 8h 16h 24h 8h Aigu: freinage Cortisol/ACTH CRH Corticoïdes Atrophie corticotrope ACTH Atrophie corticosurrénalienne Chronique: freinage Cortisol/ACTH + Atrophie
ARRET DES CORTICOIDES après corticothérapie chronique à dose freinatrice CRH Atrophie corticotrope ACTH Atrophie corticosurrénalienne ACTH 8h 16h 24h 8h Insuffisance surrénale -à l’état basal -ou à l’occasion d’un stress
Insuffisance surrénale post-corticothérapie Dose de Corticoides (avant l’arrêt) > 30mg/j équivalent hydrocortisone > 7,5 mg/j prednisone (Cortancyl Solupred) Durée de la corticothérapie > 3 semaines
Insuffisance surrénale post-corticothérapie : Manifestations cliniques Asthénie Troubles digestifs: anorexie, nausées, vomissementts Amaigrissement Hypotension Manifestations biologiques +/- Hyponatrémie Kaliémie Normale
Insuffisance surrénale post-corticothérapie Diagnostic Cortisol plasmatique <200 nmol/l à l’état basal ou <580 nmol/l sous stimulation/ Synacthène Atrophie corticotrope Atrophie corticosurrénalienne Test Synacthène : 1 ampoule 250ug IVD dosage Cortisol T0 et T60 minutes
Insuffisance surrénale post-corticothérapie Prévention Si Corticothérapie >7,5 mg/j pendant >3 semaines et quand Corticothérapie arrêtée ou baissée<7,5mg/j Dosage Cortisol plasmatique (F) à 8h du matin (après arrêt 24h corticoides) F<200 nmol/l: risque d’ISA: traitement substitutif F>200 nmol/l: test au Synacthène -T60 F>580 nmol/l: pas de risque d’ISA -T60 F<580 nmol/l risque d’ISA quand stress traitement substitutif
Baisse de la corticothérapie Equivalent Hydrocortisone 240mg (60mg prednisone) Rebond de la maladie ISA 60mg 30 mg 7,5mg prednisone
Insuffisance surrénale post-corticothérapie Traitement substitutif -Hydrocortisone état basal 20mg/j (1-1-0) per os Stress mineur (fièvre) 40 à 60 mg/j Troubles digestifs voie IV Stress majeur (Chirurgie) 200 mg/j IV -Carte d’insuffisant surrénalien -Retester tous les 3 mois
Insuffisance surrénale post-corticothérapie Traitement substitutif par hydrocortisone F (Cortisol) 8h 16h 24h 8h CRH ACTH - F +